
Airway Complications After Lung Transplantation
Michael Machuzak, MD
Department of Pulmonary, Allergy, and Critical Care
Respiratory Institute
Cleveland Clinic
Laura Frye, MD
Department of Pulmonary and Critical Care
Transplant Institute
University of Chicago
Introduction
Lung transplantation presents a unique challenge when compared to other transplanted organs for a variety of reasons. Dual blood supply with a lack of a vascular re-anastomosis, a contaminated site, medication, physical factors, as well as surgical techniques all play a role in development of airway complications (AC). Airway necrosis, dehiscence, stenosis, malacia and infections collectively make up the spectrum of airway complications and have been a significant and persistent source of morbidity and mortality since the original lung transplant. The reported rate of anastomotic complications ranges from 1.6% to 33%, although most agree with an incidence of approximately 15%-18%.1 Many potential reasons exist for this wide range; the lack of a standardized grading system may contribute significantly. Approximately 35% of patients with a previously treated airway complication will experience a second, and the chance of three or more after the second is approximately 70%.2 Frequent office visits, the need for procedures, hospitalizations, and additional medications can be a financial and time burden and minimize the perceived benefit of transplant.
The recognition and management of airway complications varies based on the time from transplant, location of the lesion, and severity. Institution specific protocols also account for variance in surveillance, diagnosis, and management. Complications can be classified temporally (early or late), by cause (ischemia, infection, iatrogenic, or idiopathic), anatomically (anastomotic or post-anastomotic), or descriptively (necrosis, dehiscence, fistula, infection, stenosis, granulation tissue or malacia). This article reviews a brief history of transplant airway complications, transplant-specific anatomy and surgical technique, risk factors for AC, classification of AC and management strategies for the various types of complications.
Risk Factors
The etiology of AC is undoubtedly multi-factorial. Surgical factors and ischemia of the donor bronchus was initially felt to be primary driver, however more complex interplay between donor and recipient characteristics, surgical technique, post-operative recovery, infections, and medication selection play a role.
Risk factors for the development of AC have been identified; including procurement after extended donor mechanical ventilation (50-70 hours) as well as taller recipients.3 Taller recipients are likely related to surgical technique, as the airway is telescoped with intussusception leading to entrapment of organisms and an increased ischemia risk.
Indications and Planning: Necrosis and Dehiscence
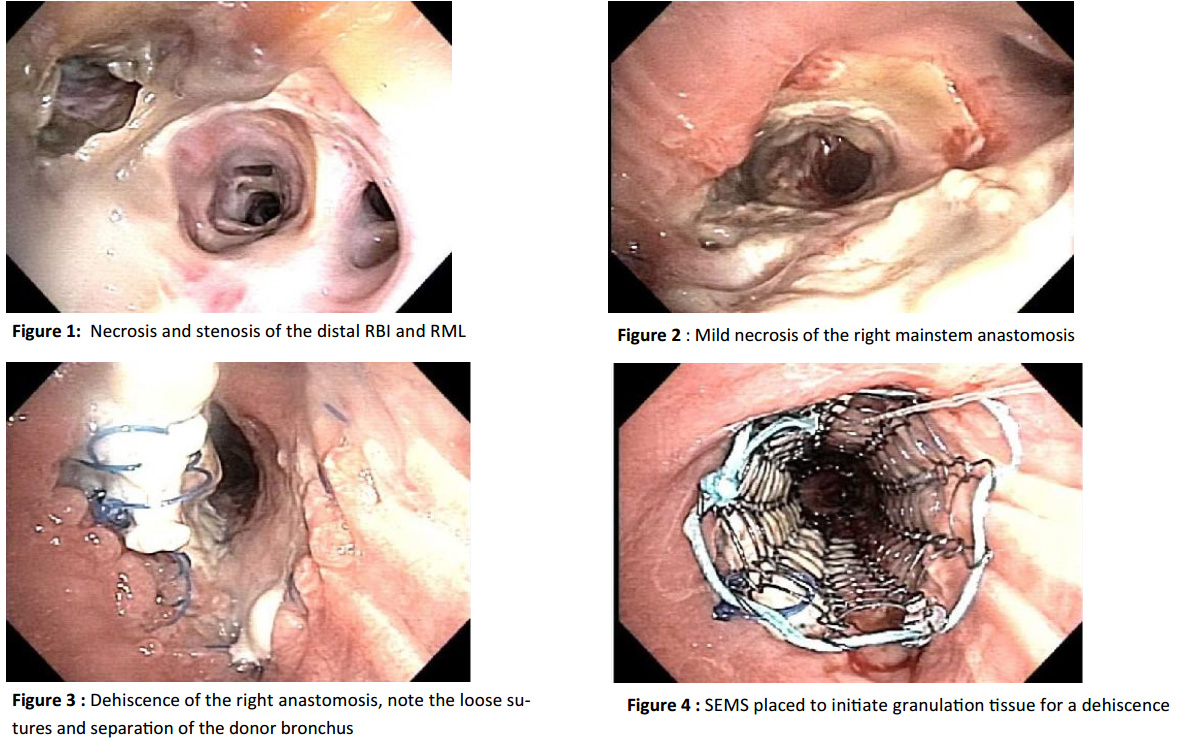
Post-transplant airway necrosis related to ischemic injury is common. The mucosal slough can extend from the anastomosis to lobar or segmental levels (Figure 1, 2). Necrosis typically resolves by the sixth week post-transplant and dehiscence occurs when normal healing fails (Figure 3). Necrosis and dehiscence represent a continuum from healing to catastrophic airway complications. True dehiscence is uncommon but rates are reported from 1- 24%, the lack of standardization complicates this.4
Bronchial dehiscence is often seen at surveillance bronchoscopy but must be considered with a prolonged air leak, spontaneous pneumothorax, failure to wean, or sepsis. Chest radiographs are unreliable. Computed tomography may be helpful showing bronchial wall defects, airway debris, or extra luminal air consistent with dehiscence but bronchoscopy remains the gold standard.
A full review of medications is too detailed for this brief piece but Sirolimus merits discussion. It is a potent immunosuppressive and antiproliferative with less renal impairment, appealing for lung transplantation. Catastrophic airway complications occurred when used in the early postoperative period. Two separate studies of sirolimus in de novo lung transplant patients describe severe wound-healing complications
with dehiscence, one resulting in a fatal event. Present recommendations are to delay using Sirolimus until complete bronchial wound healing, typically 90 days after transplantation.5,6
Mucosal slough without necrosis of the bronchial wall may respond to a conservative approach or surveillance and as needed debulking. Often antibiotic or anti-fungal regimens, including inhaled therapies, are initiated. When healing fails and dehiscence occurs, either a surgical or bronchoscopic intervention is required. Both have associated morbidity and mortality. Surgical options include reanastomosis, flap bronchoplasty, and rarely retransplantation. Bronchoscopic techniques include cyanoacrylate glue, growth factors, and autologous platelet-derived growth factors; however the overall success is poor.7
A novel technique of placing an uncovered self-expanding metal stent (SEMS) temporarily to facilitate healing exists. This technique utilizes the tendency for SEMS to initiate granulation tissue formation. The SEMS is deployed across the dehiscence and once granulation tissue and epithelialization occurs a stent exchange (if the defect is still present) or removal (if healed) is performed, typically within a few weeks (Figure 4). Mean time to stent removal was 37.5 days.8 Precise placement and removal make this method challenging with the potential to extend the injury. Close surveillance is recommended given the tendency for stenosis or malacia to occur at or distal to the site of prior dehiscence.
Fistula
Bronchial fistulae are challenging but fortunately rare and can occur as communications between the airway, pleura, mediastinum, or vasculature. Fistula may present as dyspnea, sepsis, pneumothorax, subcutaneous emphysema, or a persistent air leak typically in the setting of dehiscence. Management is similar to that of anastomotic dehiscence. Success depends on the location and size of the defect.
Bronchovascular fistulas are rare and often fatal. Erosion from any infection, particularly aspergillus, is most typical. A herald bleed must be evaluated quickly. Case reports of surgical management with pneumonectomy (if bilateral transplantation), bilobectomy, or fistula resection and reconstruction have been successful.9
Anastomotic infections
Infectious complications are common, particularly in the first 3 months, and will be seen in nearly seventy-five percent of transplant recipients with bacterial pneumonia being most common. Immunosuppression, ischemic complications, impaired mucociliary clearance, impaired lymphatic drainage, poor cough reflex due to denervation, and the direct communication of the allograft with the environment all play a role.10 Pre-transplant colonization is also common.
Infections at the anastomosis are a complication but more importantly are often the precursor to issues covered later. Diagnosis usually occurs at bronchoscopy. Inflammation, ulceration, or pseudomembranes are often seen along the airway and are treated with debridement and antibiotics. Protocols vary by institution and include systemic and inhaled regimens with voriconazole, itraconazole, and inhaled amphotericin commonly used.
Bronchial Stenosis
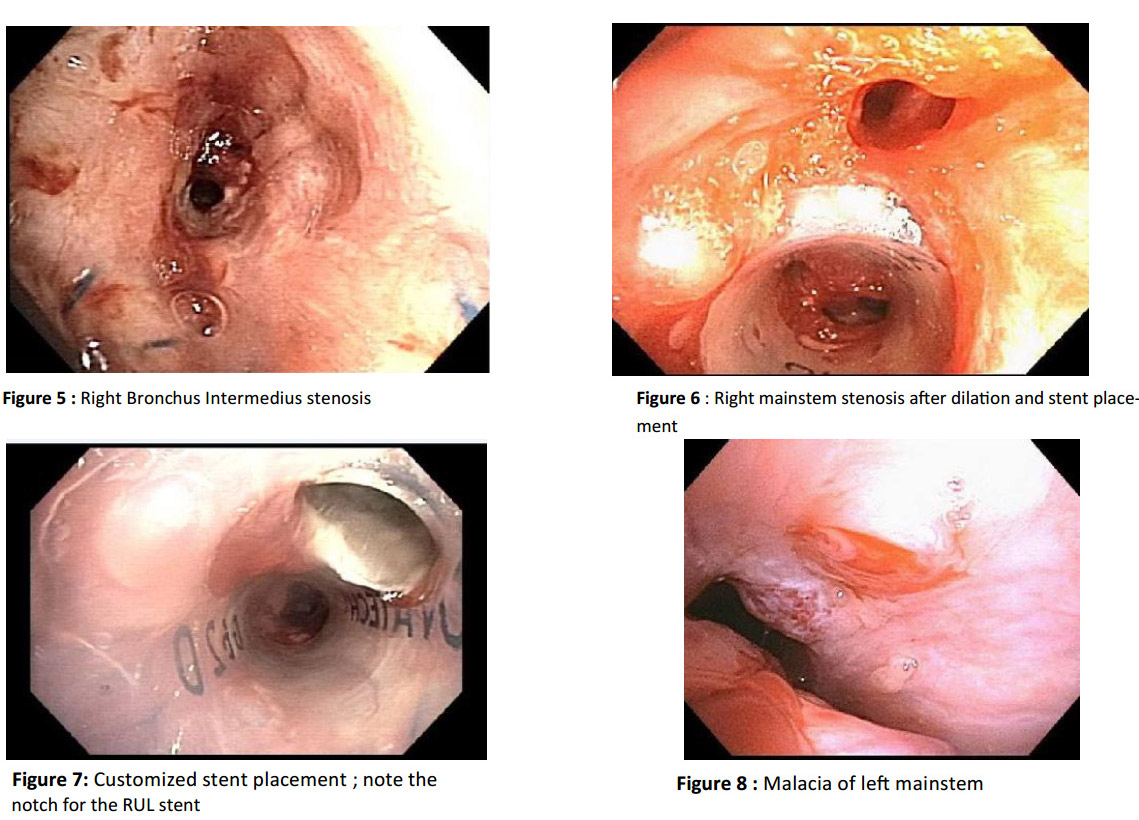
Bronchial stenosis is the best described complication; with reported rates ranging from just over 1% to as high as one third.1 They can be anastomotic or distal. (Figure 5). Non-anastomotic stenosis can be technically challenging as they can extend into segments. The bronchus intermedius is the most commonly involved non-anastomotic site, referred to as vanishing bronchus intermedius syndrome (VBIS).11
The etiology may involve infection, inflammation, or ischemia and can result in remodeling. Patients present with dyspnea, drop in spirometry, cough, wheeze, or recurrent episodes of pneumonia. Chest radiography can be the first indicator with luminal compromise or atelectasis. CT of the chest can reveal fixed bronchial narrowing. Diagnosis by flexible bronchoscopy remains the gold standard.
The management of bronchial stenosis often requires a stepwise, multimodality approach. Successful techniques include dilation, ablation, and stent placement. Dilation can be by balloon or rigid dilation. Dilation by balloon is often the first therapeutic maneuver performed and provides excellent results with relief of symptoms and improved spirometry. The stenosis often recurs after dilation, but repeated balloon dilations may be the only intervention required in 26% of cases.12 While no studies have compared methods, balloon dilation has several advantages. It can be performed via flexible bronchoscopy and under conscious sedation. Balloons come in multiple sizes and lengths allowing for specific selection. Lastly, balloon dilation allows for a rapid increase in the size of the balloon rather than repeated upsizing of the rigid bronchoscope. Rigid dilation has several advantages over balloon bronchoplasty such as expense (offset by the need for general anesthesia), direct visualization during dilation and uninterrupted ventilation. Perhaps the largest benefit of the rigid bronchoscope is the ease of stent placement if a silicone stent is to be placed.13
In cases where a focal web-like stricture is found, a mucosal sparing technique such as electrocautery or laser should be employed followed by dilation. Techniques reported include those previously reported including: cryotherapy, electrocautery, argon plasma coagulation, laser, brachytherapy, or photodynamic therapy.13
Topical applications of mitomycin-c or submucosal applications of steroids have also been used. There are no controlled trials of these interventions, however literature supports that the use of these therapies may potentially delay the time to re-stenosis.14
If the stenosis is recurrent, stenting may be required. This is a difficult decision as stent complications can be significant. The technical aspects of a complicated anastomosis has led some to favor placement of self-expanding metal stents (SEMS) However, while SEMS provide immediate relief as well as some protracted success they are fraught with long-term complications and must be carefully considered.7,8
The issues with SEMS make silicone stents generally favored for the management of benign stenosis as they have advantages of the ease of repositioning, removal and reduced granulation tissue formation (Figure 6). They are more prone to migration and require rigid bronchoscopy for placement and removal but can be customized to length, diameter or “notched” on site (Figure 7). Data suggests no increase in complications of customized stents for complex airway diseases.15
Issues with stent placement and complications have led to the development of new technologies, including 3-D printed or biodegradable stents (BDS). Biodegradable stents are well tolerated and completely dissolve after months. In one prospective study of BDS, eleven stents were placed in ten patients. All had improved spirometry and airway patency was achieved in 9/11 at 1-year follow-up with complete degradation after 141 days. 16 3-D reconstructed stents may play a role in transplant airway complications as they allow for a personalized fit.
In patients with recalcitrant stenosis alteration of immunosuppression with the addition of sirolimus can be considered (once airway healing has occurred). A retrospective review of 10 patients with recurrent stenosis reported 8 of 10 patients achieved airway patency within 3 months and 7 of 10 had a significant response within the first month of starting rapamycin.7,8
A multidisciplinary approach is ideal and if endoscopic therapy fails, a surgical approach should be considered. An invasive approach is risky but sometimes required, with bronchial anastomosis reconstruction, bronchoplasty, sleeve resection, lobectomy, pneumonectomy, and retransplantation all described.
Excessive Granulation Tissue
Occluding endoluminal granulation tissue occurs in up to a quarter of lung transplant recipients, most commonly at the anastomosis. Airway infection, particularly with aspergillus, can exaggerate this.17 Progressive dyspnea, cough, difficulty clearing secretions, post-obstructive pneumonia, or hemoptysis may be the presenting symptoms. Reduced spirometry or a chest CT showing obstructive granulation tissue may be seen but bronchoscopy remains the gold standard.
Forceps can remove granulation tissue easily, but in some cases the beveled edge of the rigid bronchoscope is required to quickly restore patency. Heat or cold modalities as well as the micro-debrider can be used to restore patency. A superior safety profile, the cryosensitivity of granulation tissue, excellent hemostasis and the ability to use around stents without the risk of ignition even in high concentrations of oxygen make cryotherapy an appealing option. APC, electrocautery, and laser ablation have a long history of successful management. High dose rate (HDR) endobronchial brachytherapy, or photodynamic therapy have also been reported but should be used with extreme caution as serious complications including fatal hemoptysis, have been described.18
Endobronchial application of antifibrotics (Mitomycin) or injection of anti-inflammatory agents has been described in the management of granulation tissue with limited success. Although randomized trials are lacking, anecdotal success and excellent safety profile encourage continued usage. Bronchial stents have been reported to improve patency in refractory cases but can promote granulation tissue. Stent placement is complicated by granulation in 12 to 36% of patients.19
Tracheobronchomalacia
Malacia of the airway presents in a myriad of ways. A “barking” cough, difficulty clearing secretions, or a drop in spirometry more marked during expiration are typical. Significant malacia is defined as luminal narrowing of 50% or more on expiration (Figure 8).20
The management is extrapolated from the non-transplant population. Aggressive pulmonary hygiene, mucolytics, and non-invasive positive pressure ventilation are tried first. Stenting may improve spirometry if medical management fails. Stenting should be carefully considered.11 If pursued, silicone stenting is typically preferred by experts with close surveillance and often a stent-free trial after 6-12 months.
Quality Control: Classification of Airway Complications
A potential reason for the wide range of reported AC may be the lack of a standardized, well-accepted grading system. Early grading systems relied on bronchoscopic inspection with some excellent findings including prediction of subsequent anastomotic complications; however they were subjective and captured only early complications. This shortcoming was later addressed. Subsequent additions included bronchial strictures, suture status, and presence of granulation tissue, dehiscence or malacia. The most recently proposed system, by Dutau and colleagues known as the MDS grading, approaches AC in a slightly different manner. Unique to this approach is the ability to include the extent of the abnormalities, from the suture line to more distal lobar and segmental levels. The M designation describes the macroscopic appearance ranging from normal healing to include cartilaginous protrusion, granulation or necrosis. The D classification describes airway diameter and the S designation assesses the suture line for dehiscence and ranges from the absence to a full dehiscence.21
A universally accepted classification system is the first step allowing for scientific study and consistent reporting to truly define the incidence, prevalence, morbidity and mortality. A taskforce of the International Society of Heart and Lung Transplant has recently completed such a classification system with results soon to be published.
Bronchial Artery Revascularization
Routine lung transplantation does not reestablish bronchial artery circulation leaving the anastomotic site dependent on retrograde flow. Anastomosis of bronchial arteries has been successful with promising short and long term results. A pilot study at the Cleveland Clinic looked at a series of 131 lung transplant patients who underwent BAR with an overall success rate of 90% including a 95% success in bilateral transplants. Bronchial artery patency was associated with uniformly normal airway healing. The 5 and 10-year survival for bilateral lung transplant was superior for BAR patients. A higher risk of bleeding was seen, not affecting safety.22 While encouraging, multi-center studies are needed to establish these benefits.
Summary
In patients with advanced pulmonary disease, lung transplantation can improve survival and quality of life. However, airway complications remain a major obstacle with associated morbidity and mortality. Patients with AC need additional visits, procedures and adjustments of medications. The increased need for care in an already complicated regimen can lead to a lower perceived improvement in quality of life. This can be discouraging, costly, and time-consuming. Recent improvements in donor and recipient selection, surgical technique, perioperative management, and immunosuppression have decreased the incidence of AC.
The management of lung transplant associated airway complications is complex. Many therapeutic options exist and there is no strong data to suggest one is superior. Management is best delivered in a multidisciplinary approach performed by individuals experienced in the above techniques with an understanding of the intricacies of the post-transplant patient.
References
1. Machuzak M et al. Curr Opin Organ Transplant 2010; 15: 582-7
2. Murthy S et al. Ann Thorac Surg 2007;84: 401-9
3.Van De Wauwer C et al. Eur J Cardiothorac Surg 2007; 31: 703-10
4. Garfein ES et al. J Thorac Cardiovasc Surg 2001; 121(1): 149-54
5.Groetzner J et al. J Heart Lung Transplant 2004; 23(5): 632-8
6.King-Biggs MB et al. Transplantation 2003; 75(9): 1437-43
7. Maloney JD et al. Ann Thorac Surg 2001; 82(6): 2109-11
8.Mughal M et al. Am J Respir Crit Care Med 2005; 172: 768-71
9.Knight J et al. J Heart Lung Transplant 2008; 27: 1179-85
10. Ahuja J et al. Radiol Clin North Am 2014; 52(1): 121-36
11. Santacruz JF et al. Proc Thorac Soc 2009; 6(1): 79-93
12. Chhajed PN et al. Chest 2001; 120(6): 1894-9
13. Machuzak M. In: Principles and practice of interventional pulmonology. New York: Springer Science + Business Media; 2013. p463 14. Cosano-Povedano J et al. J Bronchology Interv Pulmonol 2008; 15(4) 281-3.
15. Breen DP et al. Respiration 2009; 77(4): 447-53
16. Fuehner T et al. Transplant International 2013; e58-60
17. Mulligan MS. Chest Surg Clin N Am 2001; 11(4): 907-15
18. Tendulkar RD et al. Int J Radiat Oncol Biol Phys 2008; 70(3): 701-6
19. Saad CP et al. Transplantation 2003; 75(9): 1532-8
20. Simoff M et al. Thoracic endoscopy. Advances in interventional pulmonology. Malden (MA): Blackwell Publishing; 2006
21. Dutau H et al. Eur J Cardiothorac Surg 2014; 45: 33-38
22. Petterson, GB et al. Curr Opin Organ Transplant 2010; 15: 572-7









