
 Mechanical Dilatation of Benign Laryngotracheal and Tracheobronchial Strictures without Laser or Electrocautery Assistance
Mechanical Dilatation of Benign Laryngotracheal and Tracheobronchial Strictures without Laser or Electrocautery Assistance
By Antoni Rosell, MD, PhD
Assoc. Professor Universitat de Barcelona
Head of Respiratory Endoscopy Unit, Pulmonology Department
Hospital Universitari de Bellvitge, Barcelona
Introduction
Tracheobronchial strictures are the consequence of abnormal remodeling after an initial injury of the respiratory mucosa by d ifferent factors. The most frequent are ischemia, infection, trauma and surgery, while radiotherapy, caustic or thermal inhalation injuries, vasculitis and toxic gases have been less commonly reported. A combination of medical, endoscopic and surgical treatments are available to restore central airway patency. When the bronchoscopic approach is indicated, rigid scopes, balloons, bougies1 and rigid scissors2 are an option for reopening the airway strictures without inducing the thermal damage associated with thermal techniques such as lasers and electrocautery. Mechanical dilatation has to be to performed with minimal trauma, as it can also lead to recurrence of fibrotic tissues and granulation tissue formation.
Indications
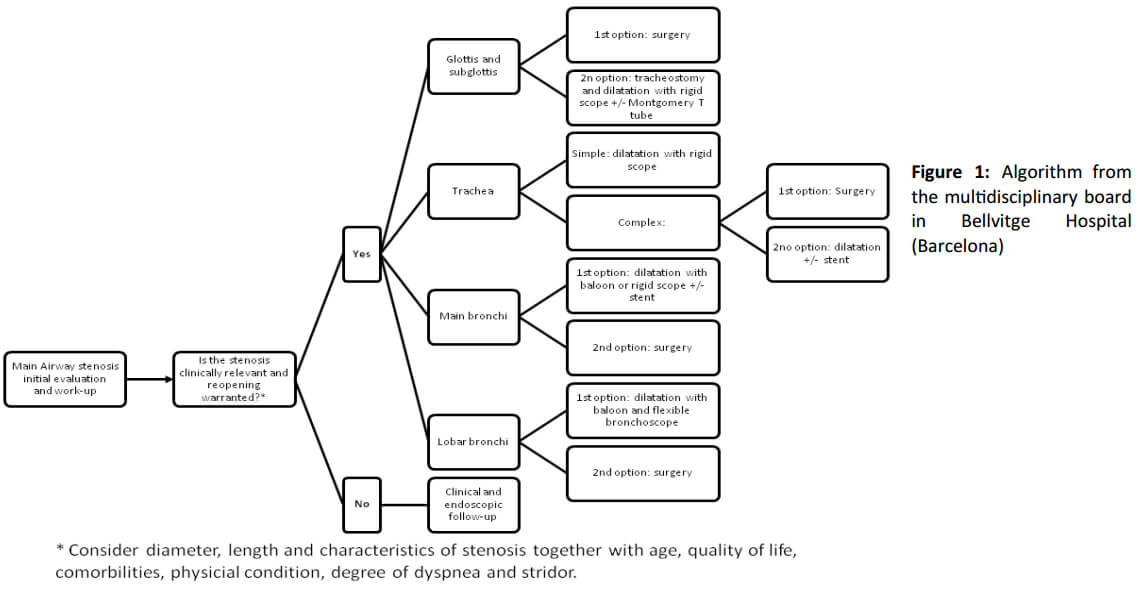
At our institution, a multidisciplinary team consisting of interventional pulmonolgists, thoracic surgeons and ear, nose and throat (ENT) surgeons, determines by consensus the best therapeutic option for each patient, following an established protocol. A multimodal approach is used based on location, tracheobronchial mucosa appearance, the length and diameter of the stenosis, and airway wall involvement3,4. Mechanical dilatation is indicated in the following 5 situations: in simple non inflammatory tracheal and bronchial stenosis, when intubating patients previous to surgery for complex stenosis, whenever surgery is not indicated, and in inoperable patients or for those not willing to be operated. For complex stenosis, the choice to additionally insert a silicone stent, a Montgomery T-tube or a tracheal cannula is case dependent (Figure 1).
Planning
Whenever possible, patients are studied in an outpatient clinic and discussed by the multidisciplinary team. The “Four Box” p ractical approach, which includes an initial evaluation, procedural strategies, procedural techniques and a long-term management plan, is followed5. The initial evaluation includes:
- A structured interview in which all potential causes of tracheobronchial benign strictures are reviewed before considering it to be an idiopathic case. Patients’ quality of life, preferences and expectations are assessed and documented.
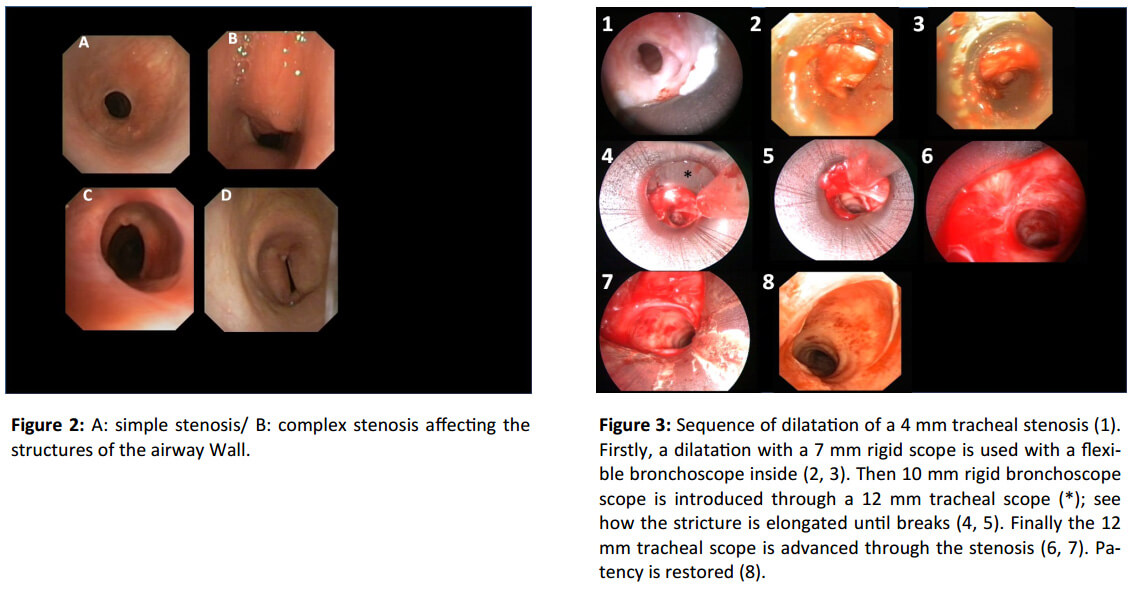
- A flexible bronchoscopy is mandatory to check laryngeal function, to determine the stricture’s morphology (i.e., triangular, circumferential, or elliptical), length, visual degree of free lumen, location and distance to vocal cords and main carina. It is also valuable to observe the aspect of the mucosa and to check for the presence of malacia, and to obtain a bronchial washing for microbiologi cal sampling (bacteria, fungi, MRSA, Klebsiella rhinoscleromatis) (Figure 2). Images and video recordings are obtained for documentation. In cases of severe stenosis presenting with a diameter of 5 mm or less, an ultrathin scope (≤ 3 mm) is recommended to a void respiratory impairment and barotrauma.
- A chest CT provides information on the morphology of the stricture and, potentially, on the degree of wall involvement. When malacia
is suspected or requires confirmation, inspiratory and expiratory images are taken. A chest CT also reveals any parenchymal/ interstitial changes that may suggest the etiologic diagnosis. 3D reconstructions are performed using a virtual bronchoscopy program. - Pulmonary function tests are directed to confirm the presence and degree of central airway obstruction through flow -volume loop
examination and maximum ventilatory ventilation (MVV). The FEV1 is a robust variable that has to be balanced against the degr ee of stenosis. In some patients, cardiopulmonary exercise testing is desirable to quantify stenosis-related effort intolerance. - Planning also includes prescribing medications with corticosteroids, antibiotics or proton pump inhibitors, as required. In all patients,
we use a single dose of 1mg/kg of predinsolone 24h before the rigid bronchoscopic procedure. - Preoperative assessment by an anesthesiologist to assess the operability of the patient is also required.
Once this information is gathered, the following two dimensions are considered:
- The disease: stenoses are classified in two categories: simple (≤1 cm in vertical length, not affecting the wall, not loca ted in larynx and non inflammatory) and complex if any of the simple features are not present. Airway wall involvement covers a broad spectrum that includes the fracture of cartilage (secondary to percutaneous tracheostomy or traumatic rupture), mural chronic inflammation wi th or without condritis, hourglass-like contracting scarring, malacia or fistula.
- The patient: operability and preferences are taken into account.
Techniques and Instrumentation
1. When treating very severe subglottic stenosis, especially for highly located lesions, a preventive tracheotomy is recommen ded to preserve ventilation in cases of post procedural excessive inflammatory narrowing of the larynx lumen.
2. For subglottic and tracheal strictures, serial dilatation with rigid bronchoscopes is our first choice. EFER-Dumon (EFER Endoscopy, La Cio-
tat, France) scopes with external diameters of 7, 8, 10, 12 and 13.2 mm are selected according to the stenosis free lumen. As a general rule, we take the scope that slightly exceeds (1-3 mm) the free lumen, so that no excessive injury to the normal mucosa is produced. The rigid telescope (available from 3.5 mm to 5.5 mm in diameter) and the suction catheter have to adapt to the inner lumen of the bron choscopes. Occasionally, a flexible bronchoscope inside the rigid bronchoscopes can be used instead, but in that case two proceduralists are required. Careful insertion of the tip of the bronchoscope into the stenosis, using a rotating motion and gentle forward pressure, typi cally results in successful advancement of the scope through the lesion (Figure 3).
To avoid perforating the tracheal wall, it is crucial to maintain the central axis while advancing the scope. When hard fibro tic tissue is encountered and it is difficult to open, one to three radial incisions with rigid scissors avoiding the posterior wall and norm al cartilage are performed to release the tension in the stricture before dilation (see video in http://www.bronchotraining.org/spip.php?article54 ). Once the stenosis has been bypassed, assessment of the distal airway and aspiration of secretions are performed using a flexible b ronchoscope. During this time, the rigid scope stays in place and tamponades the bleeding surface and consolidates the disrupted fibrotic tissue. Next, a wider rigid bronchoscope is introduced until the desired lumen patency is achieved. The maneuver of dilatation with the rigid scope can partially resect the scar tissue. Before finishing the procedure, cold saline is sometimes instilled on the treated area to reduce and control bleeding and inflammation.
3. In our institution, bronchial stenosis is usually treated with high pressure balloons (for example, CRE™ Pulmonary Balloon Dilatation
Catheter, Boston Scientific, Massachusetts, USA),under fluoroscopy. The proximal and distal ends of the stenosis are marked o n the skin with radiopaque markers. Fluorosocopic guidance is facilitated by the 2 radiopaque markers at both ends of the dilating ballo ons. Balloon markers have to cover both skin markers. Balloon length is 3 and 5 cm. Although this technique lacks the tactile feedback of the rigid bronchoscope against the tracheal wall, it provides a successive, gradual dilation system based on a well defined correlation bet ween the pressure administered and the diameter obtained (for instance, 8 mm at 3 Atm to 15 mm at 8 Atm, for the 3 cm length balloon model s). We perform progressive dilatations of 1’ per diameter. One has to consider the fact that ventilation is not possible since the b alloon totally occludes the bronchial lumen.
4. Only when implanting a stent or cannula do we occasionally use the Yttrium aluminum pevroskyte (YAP) laser, which has a hi gh coagulation effect but only moderate cutting precision, either to make a radial incision or to coagulate the bleeding mucosa. Some c enters use potassium-titanyl-phosphate [KTP] laser, CO2 laser or Holmium:YAG laser, which have higher cutting precision with less scatter and shallower penetration and therefore, the risk for collateral mucosal damage and airway perforation, respectively, is lower.
5. After each dilatation, in our practice, oral corticosteroids are administered for 10 day together with nebulized budesonid e (0.5mg/ml 2 ml twice a day) for at least 1 month.
Quality Control
Elective outpatient flexible bronchoscopy is scheduled at 30 days after the procedure to assess free lumen and to consider a second dilatation. If the lumen has decreased slightly or is similar, a second dilatation is performed. After the second dilatation, anot her flexible bronchoscopy is scheduled between 30 and 90 days accordingly to the response to the second dilatation.
Again, the same criteria are used to consider a third dilatation. After the serial dilatations have been finalized, flexible bronchoscopy, chest CT and PFT are performed to objectively check the results. If the patient significatively worsens clinically and endoscopical ly between the scheduled procedures/tests, then a failure of dilatation is considered and a stent indicated. If the stenosis relapses after 2 years from the last session, new dilatations or stenting are considered.
References
1. Casal RF et al. Am J Med Qual. 2013; 28: 69-75.
1. Alvarez-Maldonado P et al. J Bronchology Interv Pulmonol. 2009;16:254-60.
2. Dumon JF. http://www.bronchotraining.org/spip.php?article54.
3. Brichet A et al. Eur Respir J. 1999;13:888-93.
4. Freitag L et al. The European Respiratory Journal. 2007;30:7-12.
5. Colt H MS. Elsevier Saunders; 2012.









