
Stenting for Tracheoesophageal Fistula

Introduction
Acquired esophago-respiratory fistula (also referred to as tracheoesophageal fistula (TEF)) is a pathological communication between the esophagus and the trachea and/or bronchus. Etiologies are either:
1) Histologically malignant: esophageal cancer (in 5-15%) or lung cancer (in <1%) (1,2), with a higher incidence in patients receiving radiation or anti-angiogenic therapy; or
2) Histologically benign: secondary to curative intent chemoradiotherapy for esophageal cancers (in ~10%) (3), indwelling stents, high tracheostomy or endotracheal tube cuff pressures, trauma, surgery, or mediastinal infections.
Typical symptoms are those secondary to contamination of the respiratory tract with oral or gastric secretions. Patients develop intractable cough, choking after swallowing or recurrent aspiration pneumonia.
Indication for stenting
Without interventions to close the fistula, survival measures in weeks (~4 weeks) as patients will expire from pneumonia and sepsis (1,2). Closure of the TEF to prevent aspiration and to potentially allow enteral nutrition is the primary goal of treatment. The approach to achieve this palliative goal is slightly different depending on the etiology of the TEF. Patient with benign etiologies should be considered for surgical (curative) options. Surgical options include esophageal exclusion by collar esophagectomy to allow the TEF to heal, or anatomical reconstruction by fistula bypass or closure. Only a minority of patients with advanced malignancies can tolerate such major surgeries that are associated with high morbidity (up to 40%) and mortality (up to 14%) (4). Therefore, endoscopic stenting is the most commonly utilized modality to palliate symptoms in these patients. There are case reports of using endoscopic clips, occlusion devices (such as Amplatzer® devices, biologic or chemical glue, septal buttons or valves), mesenchymal stem cells injection, or application of argon plasma coagulation for small (<5mm) TEFs; but none of these are currently standard of practice or have any strong evidence to support their use. Most patients requiring endoscopic interventions require either an esophageal and/or an airway stent (Figure 1). Patients with cancer who undergo stenting have improved survival (4-8 months) when compared with patients for whom stenting is not feasible (5,6).
Planning for the procedure
Fully or partially-covered esophageal stents are, in general, the preferred first step to treat non-surgical patients suffering from TEF (Figure 2). This is because esophageal stents configure better to the esophageal wall than airway stents do to the airway wall, and because of lower rate of severe complications associated with esophageal stents (7,8). Airway stenting should be employed when esophageal stenting is unsuccessful or not technically feasible (e.g. when there is a proximal obstruction that cannot be passed, or for a TEF located high in the esophagus), or in those with pre-existing airway compromise from a tumor (Figure 1A). Patients who develop respiratory compromise post-esophageal stenting, may require an airway stent (i.e. double stenting) (6,7). This complication can be prevented by synchronous bronchoscopic evaluation prior to or during esophageal stent deployment. Alternatively, an esophageal balloon can be inflated to the diameter of the stent to assess whether there will be subsequent airway narrowing. We recommend a bronchoscopy-first approach to evaluate for airway narrowing in any patient in whom worsening airway compression post-esophageal stenting is possible based on pre-procedure chest CT scan (Figure 1C).
Double stenting may occasionally be required for a very large TEF (>2cm) (Figure 1). Caution is advised with double stenting given the risk of worsening the TEF due to mucosal necrosis caused by two expansile stents pushing against each other (6,9).
In patients with an aero-gastric fistula after a gastric pull up post-esophagectomy, who are not re-do surgical candidates, airway-first stenting is preferred as gastric stenting is usually not feasible.
Technique
Self-expandable metallic stents (SEMS) are most commonly used for esophageal stenting. They should ideally extend 2 cm proximal and distal to the TEF (7). In the airway, there are no studies comparing covered/partially covered SEMS with silicone stents for this indication. There is more evidence, however, for using SEMS for both benign and malignant TEF. These stents are easier to insert (do not necessarily require rigid bronchoscopy) and have a larger inner diameter to wall thickness ratio, with better wall apposition. They are, however, more difficult to remove 2-3 months after insertion if tissue ingrowth develops and stents become embedded. Therefore, in patients with benign TEF, who may have the stent in situ for longer periods and in whom the stent may be used as a bridge to surgery, silicone stenting may be preferred. The concern with silicone stenting for TEF is the higher radial expansile force compared with any SEMS available on the market. The high radial force could theoretically enlarge the fistula. In addition, complete apposition of the silicone stents to the airway wall may be hampered by the high stiffness of these devices (compared with SEMS, which better configure to the airway morphology). SEMS may be the preferred stents in the curved and tapered left main bronchus, due to their greater resistance to buckling (angulation), an issue that becomes relevant when the fistula is associated with concurrent airway obstruction (Figure).
Straight airway stents can be employed in almost all situations except when the TEF is next to the main carina (involving lower trachea and proximal main right or more commonly, left bronchus), wherein a bifurcated stent (Y) is usually employed. Stents should extend 1-2 cm proximal and distal to the TEF. This is obviously not always feasible for a fistula in the main bronchi or bronchus intermedius (Figure 1C). In patients with TEF in the absence of extrinsic compression from tumor, stents can be slightly over-sized (diameters should exceed the native airway diameter by 10-20%), as there is no counter-pressure exerted by a mass (as would be the case in esophageal cancers) (7). In patients with airway compromise due to tumor, caution is advised with over-sizing, as these stents may not unfold after deployment or may exert excessive pressure on the mucosa, promoting granulation tissue formation or even enlargement of the fistula. The goal here should be to cover the fistula and maintain airway patency such that the post stenting airway narrowing is <50% of normal.
We do not recommend dual stenting as a standard approach unless single stenting alone is unsuccessful in covering the fistula. Some providers prefer dual stenting approach. In these patients, the airway stent should be deployed first to avoid airway compromise post-esophageal stenting. The proximal end of the esophageal stent should be slightly cephalad to the airway stent to mitigate migration risk.
Quality Control
While TEFs can be detected with thin section CT or contrast (barium) esophagrams (Figure 1B), endoscopic visualization is required for firm diagnosis, to better define extent and degree of airway narrowing during dynamic respiration, and to properly plan a therapeutic intervention. Occasionally, edematous and hyperemic mucosa may make endoscopic visualization of a small TEF difficult; intra-procedural administration of oral methylene blue may facilitate bronchoscopic TEF detection in such cases. All TEFs should be managed using a multidisciplinary approach involving at least a bronchoscopist, a gastroenterologist and a thoracic surgeon.
Esophageal stents are the preferred first-line endoscopic option because: these stents serve as downward conduits for oral secretions, the length of the esophagus allows for longer stents, the more pliable esophagus permits better apposition, and complications are not as serious as with airway stenting (8). The non-circular shape of airways and dynamic respiratory movement makes it more difficult to achieve complete apposition of airway stents with the airway wall to prevent spillage into the respiratory tract. We therefore strongly discourage the practice of stenting the airways first when there is no concurrent airway obstruction (Figure 2). In cases of tumor between the esophagus and the airways, we believe airway inspection prior to and possibly after esophageal stenting should be performed to prevent respiratory distress due to airway compression post-esophageal stenting. We also suggest that esophageal stent sizing should be limited to simply cover the fistula and not over-distend the esophagus, which could lead not only to airway compression but also posterior wall perforation.
Stenting success is assessed by symptomatic improvement and contrast esophagram (Figure 1E). Endoscopic stent surveillance to detect early complications, or assessment for TEF healing is warranted, especially for those cases in which TEF is expected to heal (histologically benign). We routinely perform surveillance bronchoscopy at 4-6 weeks after any airway stent insertion, although the evidence for this practice derives mainly from patients with airway obstruction, not TEF (10).
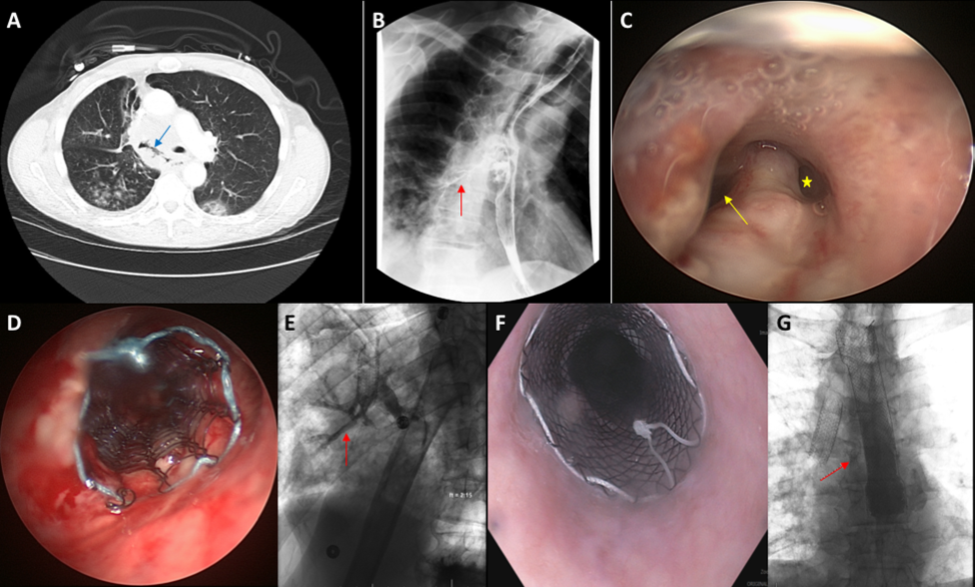
Figure 1: Post-radiation broncho-esophageal fistula seen on a CT scan (Panel A, blue arrow), with adjacent right lower lobe opacities consistent with aspiration. Esophagram demonstrated aspiration of contrast into the airways forming a contrast bronchogram (Panel B, red arrow). A large fistula in the proximal bronchus intermedius was visualized during bronchoscopy (Panel C, yellow arrow). Airway leading to the right middle and lower lobe is also seen (Panel C, yellow star). The fistula was covered with a 14 mm X 40 mm partially covered Ultraflex SEMS (Panel D). However, there was residual leak of contrast into the airway on a follow-up esophagram (Panel E, red arrow), which warranted placement of an esophageal SEMS (Panel F). Minimal leak of contrast was noted after double stenting (Panel G, red arrow).

Figure 2: * Patients with malignant TEF are rarely surgical candidates due to their poor overall health. ** A careful review of the chest CT AND pre-stenting inspection bronchoscopy allows operators to predict airway compression post-esophageal stenting. This allows the bronchoscopist to measure the extent and location of the fistula, determine length and size of the airway stent, if needed, and communicate with the endoscopy team about the potential risk of airway compression post-esophageal stenting (which may guide decision making regarding the size of the esophageal stent to be used). *** When the fistula is located in the upper esophagus, an esophageal stent may not be feasible; if there is co-existing esophageal stricture, the stent may not fully cover the fistula; sometimes, despite a careful review of the CT and pre-stenting bronchoscopy, respiratory distress can occur post-esophageal stent deployment. In any of these circumstances, an airway stent would be indicated. **** If airway stent was used first and there is a persistent leak, the stent should be inspected during conscious sedation as the stent might have migrated or have been undersized, or in the case of partially covered SEMS, there may be residual leak through the uncovered part of the stent; in any of these cases, the airway stent should be revised, if possible; if not feasible (not safe to remove it or a different stent is not technically feasible), then an esophageal stent (double stenting) should be considered. If the esophageal stent was used first, then its revision should be considered based on possibility of migration, under-sizing or residual leak through the uncovered part of the stent. If the esophageal stent cannot be revised, then an airway stent could be considered (double stenting). ***** We recommend clinical and bronchoscopic follow up at 4-6 weeks after airway stent insertion to monitor for possible stent related complications; in addition, for patients with histologically benign fistulas, if closure of the fistula is possible, the stent may need to be removed (a decision that can be taken after surveillance bronchoscopy and chest CT imaging)
References
- Burt M et al. Ann Thorac Surg. 1991;52(6):1222-8.
- Choi MK et al. Med Oncol. 2010;27(4):1234-8.
- Balazs A et al. Eur J Cardiothorac Surg. 2008;34(5):1103-7.
- Davydov M et al. Eur J Cardiothorac Surg. 2001;20(2):405-8.
- Chen YH et al. PLoS ONE. 2012;7(8):e42766.
- Herth FJ et al. Eur Respir J. 2010;36(6):1370-4.
- Hürtgen M et al. Thorac Surg Clin. 2014;24(1):117-127.
- Spaander MC et al. Endoscopy. 2016;48(10):939-48.
- Nomori H at al. Ann Thorac Surg. 2000;70(6):1803-1807.
- Lee HJ et al. J Thorac Dis. 2017;9(11):4651-4659.









