Volume 11
Issue 02
MAY 2023
Inside This Issue
Editorial, 2-4
Technology Corner, 5-7
Tips from the Experts, 8-10
Humanitarian News, 11-14
Best Image Contest, 15
WABIP News, 16-20
Educaon, 21
Research, 22-23
Links, 24
Stefano Gasparini
Chair of WABIP (Ancona, Italy)
Silvia Quadrelli
Chair of WABIP Membership Commiee (Buenos Aires,
Argenna)
Vision and Future Direction of the WABIP
WABIP Newsletter
M A Y 2 0 2 3 V O L U M E 1 1 , I S S U E 2
EXECUTIVE BOARD
Stefano Gasparini, MD
Italy, Chair
Pyng Lee, MD, PhD
Singapore, Vice-Chair
Hideo Saka, MD
Japan , Immediate Past-
Chair
Silvia Quadrelli, MD
Membership Commiee
Chair
Jean-Michel Vergnon, MD
Educaon Commiee
Chair
Ali Musani, MD
Finance Commiee Chair
Naofumi Shinagawa, MD
Japan,
Secretary General
Menaldi Rasmin, MD, PhD
Indonesia , President
WCBIP 2024
Rajesh Thomas, MD, PhD
Melbourne , President
WCBIP 2026
STAFF
Michael Mendoza
General Manager
Judy McConnell
Administrator
Kazuhiro Yasufuku
Newsleer Editor-in-chief
P A G E 2
The World Associaon for Bronchology and Intervenonal
Pulmonology has traveled a long road, dening and being
dened by the history of bronchology procedures them-
selves. This organizaon, formerly known as the "World
Associaon for Bronchology" (WAB), was created in Japan
in 1978 by Dr. Shigeto Ikeda, a Japanese thoracic surgeon
and bronchologist. In the late 1960s, he was responsible
for the creaon of the exible beropc bronchoscope
and was the rst Chair of the Associaon.
Thanks to the development of bronchoscopy and related
techniques, which became essenal in the diagnosc-
therapeuc pathways of many respiratory pathologies, the
WAB grew with the adherence of many colleagues from
dierent parts of the world. In this process of growth, the
work of various Chairs who succeeded Dr. Ikeda
(Professors Hirokuni Yoshimura, Udaya Prakash, Pablo
Diaz Jimenez, Hiroaki Osada, Henri Colt, Zsolt Papai, Silvia
Quadrelli, and Hideo Saka) was fundamental.
Major changes in the organizaon of the Associaon were
made in 2010-2012. The name of the organizaon was
changed to "World Associaon for Bronchology and Inter-
venonal Pulmonology" (WABIP) to include not only bron-
choscopy but also all the procedures (e.g., thoracoscopy,
pleural drainage, esophageal procedures) that are within
the competence of Intervenonal Pulmonology.
Furthermore, in an eort to be more inclusive and trans-
parent, an idea of Henri Colt approved by the Board of
Regents led to the adopon of a new membership modali-
ty. No more single membership, but the inclusion of Mem-
ber Sociees (naonal, regional, or local pulmonology or
intervenonal pulmonology sociees or groups). This
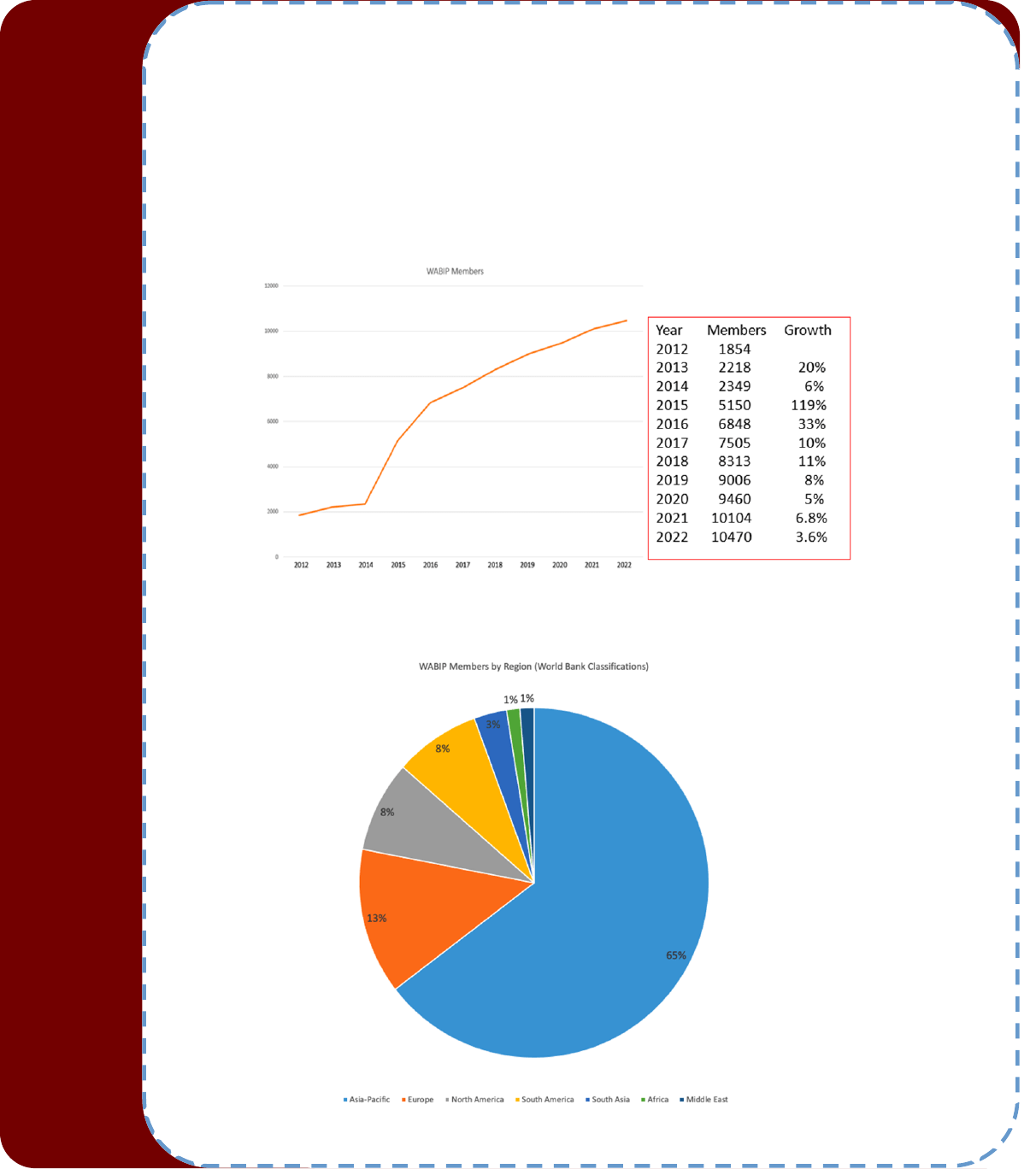
change in membership modality allowed the adopon of a
signicantly reduced cost, facilitang relaonships with
many naonal pneumological associaons and expo-
nenially increasing the number of Members from 2014
(Fig. 1). Fig. 2 shows the distribuon of WABIP Members by Re-
gion.
WABIP has already played a vital role in promong the discipline
of Intervenonal Pulmonology and enhancing paent care, parc-
ularly in naons with limited access to educaon. In addion to its
mission of bringing together healthcare professionals interested in
Intervenonal Pulmonology and providing them with opportuni-
es for networking, educaon, and collaboraon, WABIP has de-
voted the majority of its eorts to ensuring that all intervenonal
pulmonologists around the world possess a minimum level of skills
and knowledge. The operaons of WABIP are based on the belief
that medical educators have a responsibility to democraze
knowledge. WABIP views its purpose of enhancing the abilies of
intervenonal pulmonologists as a means to promote the health
and well-being of paents around the world, in light of its belief
that access to high-quality health care is a fundamental human
right. All individuals, regardless of socioeconomic status, gender,
race, ethnicity, religion, or geographic locaon, should have equal
access to high-quality healthcare services, and the rst step in
achieving this objecve is to ensure that these individuals have
access to well-trained physicians.
With this in mind, WABIP (now with over 10,000 Members from
100 countries) has developed free standard teaching and evalua-
on tools, organized hands-on courses in basic and advanced
bronchoscopy in more than 20 countries (the last in Uruguay,
Argenna, Chile, and Ecuador), organized webinars on the dier-
ent aspects of Intervenonal Pulmonology, and provided grants
for vising professors and scholarships for rotaons in highly spe-
cialized Intervenonal Pulmonology Units for doctors working in
countries with fewer resources.
WABIP also aims to assist each member country in acquiring the
basic resources and support for research and innovaon in bron-
chology and pleural diseases.
With the aim to diuse Intervenonal Pulmonology in the world, It
must be menoned also the recent creaon of the WABIP Inter-
venonal Pulmonology Instute (IPI), thanks to the commitment
W A B I P N E W S L E T T E R
P A G E 3
For the tenth consecuve year, WABIP connues its tradion of
providing reduced subscripon rates for its ocial journals: Respi-
rology, Respiraon, and the Journal of Bronchology and Interven-
onal Pulmonology, supporng its Members with the opportunity
for connuous updates.
WABIP programs were made possible by the generosity and
seless cooperaon of specialists from a variety of naons who
trained themselves as instructors and volunteered their me,
eort, and knowledge in various communies. WABIP knows that
to ensure internaonal cooperaon is equitable, sustainable, and
respecul of the dignity and rights of individuals and communies,
it must be based on ethical values. To ensure the fundamental
ethical principles of the autonomy of individuals and communies,
WABIP is a truly democrac organizaon in which each member
country has a representave (Regent) whose vote carries the same
weight regardless of the country's size, populaon, level of bron-
chology development, or economic strength. In this way, WABIP
aempts to ensure that collaboraon is founded on partnerships
that are equitable and respecul of the needs and ambions of the
communies concerned, and not on imbalances of power.
Since the creaon of WABIP, a lot has been done, but much sll
needs to be done. We must prepare for the future that is just
around the bend. Due to developments in technology, changes in
healthcare delivery, and evolving societal needs, the future of med-
ical educaon is likely to undergo substanal transformaons. We
may need to include training in arcial intelligence, telemedicine,
and other technologies to equip our medical community for the
digital healthcare environment.
With the reorganizaon of the "Social Media Commiee," now
renamed "Media Commiee," we will try to give further visibility to
our Associaon, with the aim of involving an increasing number of
colleagues and member countries.
New webinars on the dierent aspects of Intervenonal Pulmonol-
ogy and new documents on the standardizaon of procedures are
in the pipeline, as well as the creaon of interest groups in which it
will be possible to exchange experiences and opinions on individual
cases or procedures.
WABIP must increasingly become a global community, driven and
dominated by the passion for Intervenonal Pulmonology and love
for paents suering from respiratory diseases. In spite of the fact
that Intervenonal Pulmonology is a eld that is highly dependent
on technological advancements, we must never forget that we are
human doctors who deal with human paents, make decisions,
provide human care, and preserve the rights of paents.
WABIP is well-prepared for the educaon of the future, being fa-
miliar with the most recent technological advances while at the
same me maintaining a tradion of educaonal philosophy that
will t the needs of medical educaon in the coming decades,
which will increasingly emphasize paent-centered care, making
and passion of Dr. Ali Musani. IPI aims to collaborate
with countries that have large or public private Hospital
via local WABIP members to oer Intervenonal Pulmo-
nology training and related service in the region. The IPI
will oer well-designed fellowship training with WABIP
faculty available on site for 2-4 weeks at a me with
volunteers covering the enre years. Aer training com-
pleon, the fellows will receive a cercate issued by the
WABIP and will be able to start their own program in
their Country, train more people and open more center
in the region.
Recently, substanal changes have been made to the
bylaws with the approval of the Board of Regents. Parc-
ularly, to increase parcipaon and involve the leader-
ship of WABIP in the decision-making processes, the
Chairs of the main Commiees (Educaon, Finance, and
Membership) and the Editor of the Newsleer have been
included in the Execuve Board. The restructuring of the
Execuve Board reects WABIP's commitment to staying
at the forefront of Intervenonal Pulmonology and en-
hancing the organizaon's ability to serve its Members
and promote its mission of improving paent care world-
wide.
The Execuve Board's primary responsibility is to ensure
that all WABIP acvies are designed and implemented
with cultural sensivity and respect for diversity, taking
into account the cultural values, beliefs, and tradions of
the communies involved. No educaon can be eecve
if it does not respect and safeguard the rights and dignity
of individuals and communies, including their cultural
history and identy.
WABIP Newsleer, thanks to the wonderful and great
commitment of Kazuhiro Yasufuku, serves as a vehicle
for updates, publishing in each issue a synthesis of the
newest technologies in Intervenonal Pulmonology and
praccal ps and suggesons from experts. Newsleers
are sent to more than 7,500 recipients and read online
by about 2,000 colleagues.
One of the purposes of WABIP, as a scienc associaon,
is also to propose documents and guidelines for the
standardizaon of procedures. In the past, a complete
guideline for the acquision and preparaon of conven-
onal and endobronchial ultrasound-guided transbron-
chial needle aspiraon specimens was published
(Respiraon 2014; 88: 500-517). A document on
"Proposed quality indicators and recommended standard
reporng items for EBUS bronchoscopy performance"
has been prepared by a group of colleagues, under the
guidance of Daniel Steinfort, and is ready for publicaon.
A document on airway stenng is ongoing and will be
ready soon.
W A B I P N E W S L E T T E R
P A G E 4
empathy, communicaon, and cultural competence
more signicant.
WABIP believes that by collaborang in a spirit of part-
nership, we can create a more equal and just world for
everyone. We require the assistance of each and every
Member of our Associaon. Your ideas, feedback, and
iniaves serve as the basis for our work. We call on you
to join us in our work: there is a long road ahead and
much work to be completed.
Figure 1. Number of WABIP Members from 2012 to 2022
Figure 2. Distribuon of WABIP Members by Region
W A B I P N E W S L E T T E R
P A G E 5
Technology Corner
Roboc Technology in Thoracic Surgery
Introducon
Robocally augmented surgery is becoming an increasingly essenal piece of a modern thoracic surgeon’s workow. Constant and
rapid innovaon in the eld has enabled surgeons to perform complex procedures with reliability and precision. Roboc surgery has
decreased the prevalence of open thoracotomy cases, improved paent outcomes, and reduced complicaons for many lung resec-
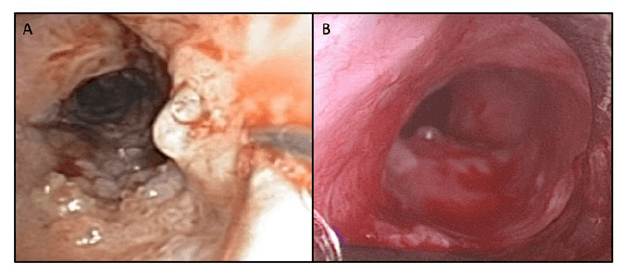
on procedures (2). Three plaorms currently available in thoracic surgery are the DaVinci Xi, Hugo RAS, and CMR Versius.
DaVinci Xi
The DaVinci Xi is a roboc surgical system that has four slim boom-mounted arms, extended reach, guided targeng, and many inte-
grated auxiliary features. This plaorm is the rst entrant to the market in surgical robocs. The adjustability of the Xi is a strong
point, with congurable paent clearance joints in each arm of the robot. The many arms of the Xi permit four-quadrant access dur-
ing surgery. The system also boasts a two-camera installaon, perming 3D view of the subject (2). The DaVinci Xi currently has
been studied in all areas of Thoracic Surgery, including lung resecon and mediasnal resecon.
Giorgio Abichedid, BSc
University of Toronto
Waël C. Hanna, MDCM, MBA,
FRCSC
Head of Division, Thoracic Surgery
Head of Service, Endoscopy
Associate Professor, Departments of
Surgery and HEI
Overview of the DaVinci Xi (intuive.com)

W A B I P N E W S L E T T E R
P A G E 6
Hugo RAS
The Hugo RAS (robocally assisted surgery) system is a modular and customizable system. Each arm is its own isolated unit, which
means it can be ed with it’s own tool and posioned to the surgeon’s specicaons for the procedure. It is less all-inclusive than
the Versius, but more versale than the DaVinci Xi. The open console also permits 3D vision of the operang eld, but requires the
operator to wear 3D glasses, which can potenally cause some discomfort (2). In terms of regulaon, the Hugo RAS has regulatory
approval in Canada for general surgery, gynecological surgery, and urological surgery. The rst cases to have ulized the Hugo RAS
were done at the University Health Network, at the University of Toronto.
CMR Versius
The Versius’ dening feature is its open console, which allows exible operaon from either a standing or seated posion (1). This is a
clear advantage as it allows each operator to work from a more comfortable posion for them. The system also includes up to 7 mod-
ular arms, although having that many is an experimental approach that has not been used in real clinical pracce. The CMR Versius,
like both previous systems, posses a 3D view in the surgeon console, although again, requires 3D glasses like the Hugo RAS. The
plaorm has been studied in preclinical trials using cadavers. Of 24 thoracic procedures were tested using the Versius, and only one
failed due to a plaorm error (4). Out of 18 lobectomies, one was not completed due to cadaver anatomy, and out of 3 thymecto-
Overview of the Medtronic Hugo RAS (medtronic.com)
Overview of the Versius Surgical System. (4)
W A B I P N E W S L E T T E R
P A G E 7
mies, one failed due to a console system error (4). All 3 diaphragm plicaons were completed without fault (4). These results suggest
condence in the Versius for robocally augmented thoracic surgery.
Discussion
Aer reviewing some of the plaorms viable for robocally augmented thoracic surgery, there are many factors to consider when
choosing a system to use.
The DaVinci Xi has the obvious advantage of me. It is the most established name in roboc thoracic surgery. It has many publica-
ons aesng to its reliability in improving paent outcomes. Clinics adopng the DaVinci Xi have found an almost 20 percent reduc-
on in post-operave complicaons (8). They also measured a general decrease in readmission and length of stay.
The Hugo RAS has not received regulatory approval yet, and would therefore tend to be a more pioneering choice for a plaorm. It
does boast some unique features, and has been proven in other elds.
The Versius has the advantage of being tested through publicly-available preclinical evaluaons, although with the caveat that they
were performed on cadavers. Other evaluaons include tesng its prociency at performing procedures in small, enclosed spaces (4).
These tests aempt to emulate the environment the Versius would be performing in, being minimally invasive thoracic surgery.
References
1. Alkatout I et al. J. Clin. Med. 2022; 11(13): 3754
2. Cepolina, F et al. Int J Med Robot. 2022; 18(4): e2409
3. Ferng, A. Meet Versius, Cambridge Medical Robocs’ Portable and Cost Eecve Robot for Minimal Access Surgery. Medgadget. 2017. hps://
www.medgadget.com/2017/11/cambridge-medical-robocs-minimal-access-surgery-versius.html
4. Giuseppe A et al. Eur J Cardiothorac Surg. 2022; 62 (3):ezac178
5. Kayser, M et al. Children. 2022; 9(2):199
6. Medtronic’s Hugo Clears 3 Major Regulatory Hurdles. 2022. Mddionline.com. hps://www.mddionline.com/robocs/medtronics-hugo-clears-
3-major-regulatory-hurdles
7. Ngu J et al. Roboc Surgery: Research and Reviews 2017;4:77–85
8. Soliman B et al. J Thorac Dis, 2020;12(7):3561-3572

Tips from the Experts
P A G E 8 V O L U M E 1 1 , I S S U E 2
Introducon:
Recurrent respiratory papillomatosis (RRP) is a benign neoplasm of the airways caused by the human papillomavirus (HPV), most commonly
type 6 and 11 but rarer types 16, 18, 31, and 33 have been reported. (1) RRP is characterized by the proliferaon of benign squamous papil-
lomas involving the aerodigesve tract. This enty predominantly aects the laryngeal structures, with the vocal cord being the commonest;
however, it can aect any areas of the aerodigesve tract and has been reported to involve tracheobronchial tree in up to 9% and pulmo-
nary parenchyma in up to 2% of the cases. (2). Management of RRP is complicated by its mulfocal and recurrent paern, requiring mul-
disciplinary and frequent intervenons. Herein we describe the procedural technique and literature to support the mulmodal treatment
approach and intra-lesional administraon of an an-VEGF agent, bevacizumab.
Background:
The natural course of RRP is variable with a small proporon of cases obtaining either spontaneous remission or persisng as stable disease
requiring periodic intervenons. Many paents, however, have an aggressive form that requires frequent local and systemic treatments. No
clear prognosc factors have been dened for worse outcomes. However, HPV type 11 has been associated with a more aggressive nature
compared to type 6. Other paent-related factors such as younger age and laryngeal involvement at diagnosis, laryngopharyngeal reux,
and smoking have all been considered as poor prognosc factors. Although a histologically benign disease, RRP is associated with signicant
morbidity and in its aggressive form, requires frequent surgical treatments primarily aimed at excision of the papillomas to restore airway
caliber and palliaon of symptoms. Several endoscopic intervenons such as microdebrider, laser surgery (KTP, CO2), argon plasma coagula-
on, and photodynamic therapy have been successfully reported in the literature. As the name implies, RRP usually follows a relapsing, re-
ming course posing a signicant burden to paents and the health system. Hence, adjuvant systemic or intra-lesional treatments are con-
sidered to potenally improve disease burden, decrease the frequency of procedures and possibly achieve remission. There are no clear
criteria for which paents might benet from addional therapies; however, the need of more than four procedures per year, rapid re-
Intra-lesional injecon of Bevacizumab for Recurrent Respiratory Papillomatosis
Sepmiu Murgu, MD, FCCP, DAABIP
Professor of Medicine
The University of Chicago
Nakul Ravikumar, MD
Fellow, Intervenonal Pulmonology
University of Chicago
Tips from the Experts
P A G E 9 V O L U M E 1 1 , I S S U E 2
growth of papilloma with airway compromise, and distal spread of the disease have been considered as factors to be considered for oering
adjuvant treatments. Literature reports that 10-20% of paents with RRP receive adjuvant treatment, with some of the opons available be-
ing an-viral agents (cidofovir, ribavirin, acyclovir), interferon, renoids and histamine blockers. (3) More recently, targeted intervenons
focusing on immune modulaon using monoclonal anbodies with checkpoint inhibion, such as an-program death ligand-1 (PDL-1) and
vascular endothelial growth factor (VEGF) inhibion, have been used.
Clinical Applicaon:
How we do it:
At our instuon, paents with RRP are evaluated by a mul-disciplinary complex airway team comprising intervenonal pulmonologists (IP),
otorhinolaryngologists (ENT), and thoracic surgeons. In cases involving both laryngeal and tracheobronchial tree, ENT and IP teams work to-
gether in a combined procedure to target both upper and central airways simultaneously. All procedures in our instuon are done under
general anesthesia using suspension microlaryngoscopy (by ENT) for treang laryngeal disease and the rigid bronchoscope for treang tra-
cheobronchial disease (by IP). A mulmodal treatment approach comprising various endoscopic intervenons such as laser surgery ulizing
CO2 (laryngeal) and KTP (tracheobronchial), microdebrider (laryngeal), and cryosurgery (tracheobronchial) with repeated freeze-thaw cycles
are used to establish adequate airway patency. Aer restoring adequate airway patency (typically less than 20-30% lumen narrowing), we
use a 25g needle for intra-lesional delivery of the an-VEGF agent, bevacizumab (37.5 mg). Sites of injecon are selected based on the areas
with high disease burden or recurrent areas aer previous treatments. Paents are followed up on an outpaent basis. This procedure is re-
peated at an interval of 3 months (for 3-4 sessions) or earlier if symptoms recur. Addional intervenons are then performed depending on
the symptoms or at scheduled 6–8-month intervals if disease response is favorable and paents remain clinically stable (Figure. 1).
Supporng literature:
Bevacizumab is a recombinant human monoclonal anbody that targets and binds to VEGF and inhibits interacon with the VEGF receptor,
prevenng angiogenesis. The inherent vascularity of papillomatosis has a potenal pathogenic role in the recurrence of these lesions, and
hence bevacizumab is being considered in the prevenon of neoproliferave growth of RRP. Bevacizumab has been used successfully in other
neovascular diseases involving the eyes, telangiectasias. Zeitels et al. combined intra-lesional bevacizumab with laser (KTP photoangiolysis)
for paents with RRP aecng the vocal cords and noted no discernible disease in 15% of the paents and overall improvement in another
85% of the paents aer four injecons (4). In another study in the pediatric populaon looking at Derkay scores (A funconal and anatomic
assessment scoring designed by the RRP task force), the me interval between injecons and voice outcomes showed an overall improve-
ment of 58% in Derkay score and all paents having increased interval between injecons. (5) Dosing of bevacizumab delivered intralesional-
Tips from the Experts
P A G E 10 V O L U M E 1 1 , I S S U E 2
ly is much less than the typical systemic dose of 5-10mg/kg and hence it is well tolerated. A safety study monitoring physiologic and lab pa-
rameters with dosing regimens varying from 10mg to 80mg per treatment episode with a median dose of 30mg did not show any systemic
side eects, and all paents tolerated the medicaon well (6).
Conclusions:
RRP is a benign neoplasm with a high morbidity and mortality secondary with only a small proporon of paents undergoing malignant trans-
formaon. Nevertheless, frequent endoscopic intervenons are the norm in the management of these paents and the addion of adjunct
local pharmacological therapies may help decrease the disease burden, avoid side eects of systemic therapy and improve the quality of life
in these paents. Hence, the ecacy of intra-lesional injecons of medicaons such as bevacizumab, or other novel therapies such as an-
PDL1 agents (avelumab) should be evaluated in mul-center, randomized studies.
References:
1. Hoesli RC et al. Otolaryngology–Head and Neck Surgery. 2020;163(4):785–90
2. Soldatski IL et al. Laryngoscope. 2005 Oct;115(10):1848–54
3. Schra S et al. Arch Otolaryngol Head Neck Surg. 2004 Sep;130(9):1039–42
4. Zeitels SM et al. Ann Otol Rhinol Laryngol. 2011 Oct;120(10):627–34
5. Sidell DR et al. Ann Otol Rhinol Laryngol. 2014 Mar;123(3):214-21
6. Best SR et al. Ann Otol Rhinol Laryngol. 2012 Sep;121(9):587-93
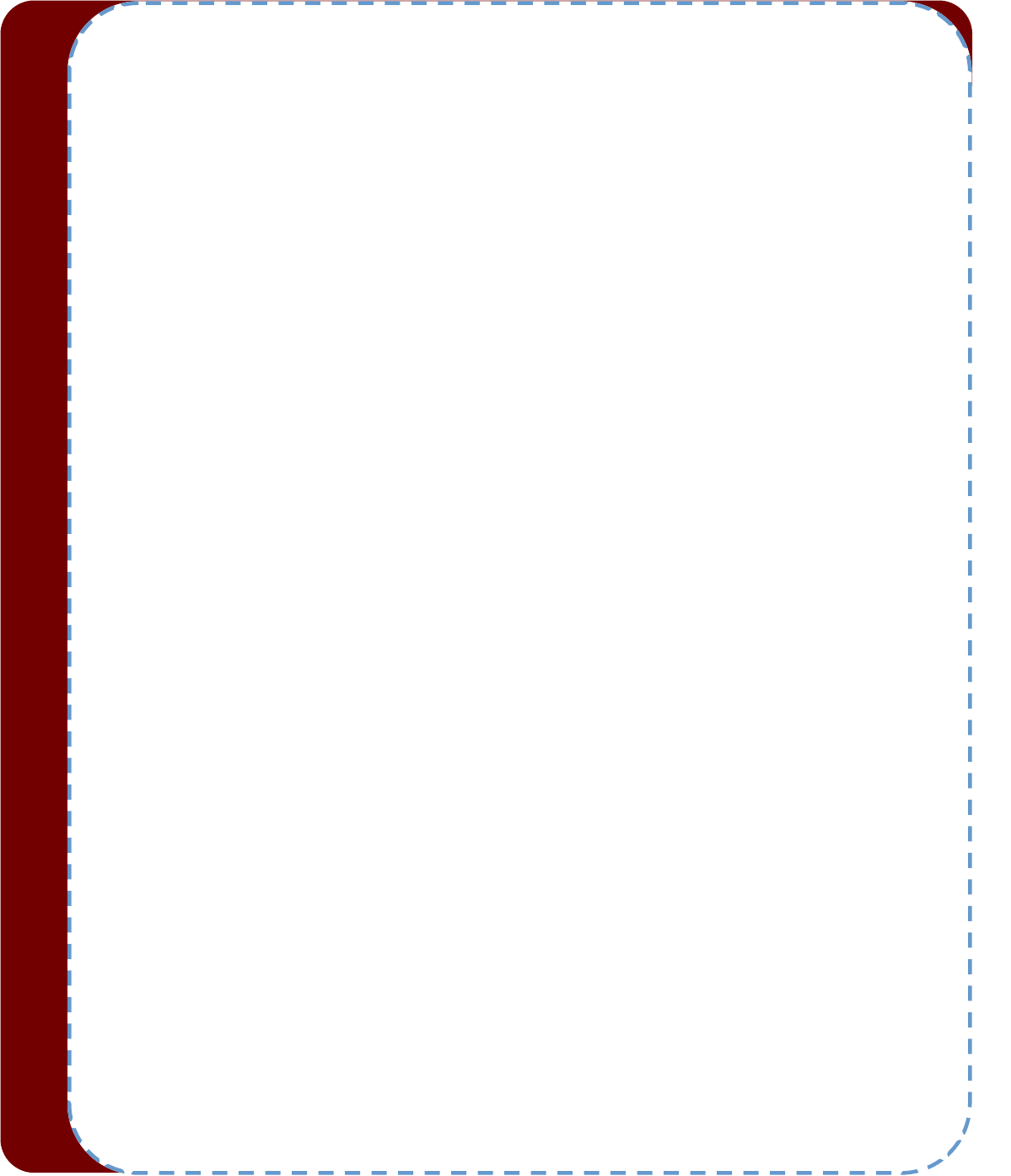
Figure. 1: Pre and post treatment of RRP with cryotherapy and intralesional injecon of bevacizumab
A: Diuse airway involvement comprising of exophyc lesions from RRP, immediately aer cryotherapy (note the diuse
blanching) At 3 o’clock posion, the needle is seen being advanced in the mucosal lesion as Bevacizumab is being injected.
B: Follow up bronchoscopy shows signicant decrease in airway papillomatosis
Humanitarian News
W A B I P N E W S L E T T E R P A G E 11
Humanitarian Aid During War Times, Challenges and Limitaons
Since the 2022 invasion of Ukraine by Russian forces, countless lives have been lost, and many more have been destroyed or
displaced by connuous shelling and air strikes. Millions of people have become refugees, and many more have been dis-
placed within the country. UN dierent agencies have reached close to 16 million people with humanitarian assistance, in-
cluding the world's largest humanitarian cash response, thousands of convoys, generator deliveries to crical facilies, and
repairs to damaged homes. Urgent needs connue, and it is ancipated $3.9 billion will be necessary in 2023 to help over 11
million people out of nearly 18 million in need.
Humanitarian workers are accustomed to the rigours of armed conicts, but the war in Ukraine presents them with unprece-
dented challenges, not only due to the severity of the humanitarian crisis, but also due to the contradicon with their funda-
mental principles of conduct. Humanitarian help is predicated on the idea of neutrality, which requires relief workers to stay
unbiased and not take sides in a crisis or polical situaon. The neutrality principle assures that aid is delivered solely on the
basis of need, without discriminaon or bias towards any parcular group or ideology. In pracse, neutrality dictates that aid
workers should not engage in any acons that could be interpreted as taking sides or favouring one group over another. Hu-
manitarian workers must maintain ght independence and avoid any polical or military parcipaon that could damage
their imparality.
The Ukraine conict will test the neutrality concept. How neutral must humanitarian organisaons remain in the face of an
allegedly unprovoked military aggression and violaons of Internaonal Humanitarian Law, lest they be accused of aiding
and abeng these abuses? How imparal are internaonal actors supported by naons polically and militarily acve in
Ukraine, including the Internaonal Commiee of the Red Cross? How does the idea that Ukrainian actors are somemes
militarily acve and oen policised aect the behaviour of internaonal actors? How should humanitarian organisaons
handle their public messaging and image when informaon is a primary weapon of war? The neutrality/parsanship conun-
drum is not new, but given the geopolical context of the crisis, its worldwide repercussions, and the connuous real-me
aenon it receives online, it may take on a bigger signicance. During the Iraq War, American Army ocers were extremely
tough on French organisaon volunteers, just as during the Kosovo War, a non-NATO passport was required to negoate
with the Serbs. But for the majority of "Western" relief workers, these conicts were far enough for them to feel able to di-
vorce the posions of their governments from their humanitarian work. But, the direct impact of the Ukraine conict on
their daily lives, the extensive engagement of their governments, and the unwavering stance of the mainstream media cre-
ate a dierent scenario.
During this conict, many humanitarian groups and the countries that sponsor them will depart from the noon of humani-
tarian neutrality, which has so dominated western humanitarian help in wars over the past three decades. Several humani-
tarians have instead chosen for polical solidarity with Ukrainians and view humanitarian help as an integral part of the
Ukrainian ght to Russian violence and oppression. It implies that some established humanitarian agencies, as well as the
majority of new ones spawned by this crisis, prefer to funcon in polical solidarity with the Ukrainian government and the
humanitarian administraon and resistance networks that emerge in response to the conict. Two tradions of humanitari-
an aid have always existed: the imparal humanitarianism culvated by the Swiss-founded Red Cross organisaon, and an
acvist legacy of opposion humanitarianism based on specic polical commitments. Throughout the 20th century, re-
sistance humanitarianism played a crucial role in rescue missions from Nazi-occupied Europe, campaigns against apartheid
and Lan American tyrants, and independence movements in a number of naons. Certain nongovernmental organisaons,
such as Médecins sans fronères, Médecins du Monde, and Prémiere Urgence, place a high priority on documenng and
reporng human rights breaches. But the concern associated with the unprecedented extent of this new viewpoint of
“solidarity” is that, while some abuses of internaonal law and human rights are evident and well-documented, the queson
of whether a parcular war is just is ulmately a maer of perspecve and interpretaon. Others may disagree with those
who believe that certain wars t the condions for a just war. And relief workers who are naonals of one of the beligerant
pares (directly or indirectly) may be signicantly impacted by the prevalent public opinion of their countries and the infor-
maon accessible in the area in which they reside, both of which are inherently skewed during warme.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 12
Mainly Western governments and mullateral organisaons have allocated or pledged billions of dollars in bilateral aid to
the governments of Ukraine and refugee-hosng countries. They are also the primary supporters of the tradional interna-
onal humanitarian network of UN agencies, Red Cross/Red Crescent groups, and internaonal non-governmental organisa-
ons (NGOs), which is mostly administered by the Oce for the Coordinaon of Humanitarian Aairs (OCHA). Similar to the
challenge of imparality, nancial sources frequently dictate where humanitarian organisaons operate. Those primarily
nanced by Western naons operate mostly in areas controlled by the Ukrainian government. They may even be instructed
to do so by their funders in order to demonstrate their support for the Ukrainian government and contribute to easing the
strain on its economy and infrastructure. On the other hand, some NGOs acvely refuse nancing from Western govern-
ments to avoid co-optaon and preserve their independence in idenfying the most urgent needs and the most eecve
responses.
The way humanitarian nance is usually channelled – from donor agencies with specic mandates to large UN agencies also
with specic mandates – will largely determine to which populaons, groups or sectors resources ow, instead of an alloca-
on based on severity of need. Western donor funding (whether labelled humanitarian or not) is likely to be deliberately
channelled to parts of the country, populaon groups or organisaons that are acvely resisng Russian forces. As a result, it
is more likely that the majority of funding will be directed to
areas where it is easiest to operate, i.e., refugee-hosng countries and government-controlled areas in Ukraine. Hard-to-
reach areas, such as those under Russian control where fewer people live, could be overlooked. This is in spite of such areas
potenally having more acute needs due to the intensity of the conict and the breakdown of naonal and local safety nets.
In Ukraine, Russia, neighbouring naons, the West, and elsewhere, governments, the media, public opinion, and humanitari-
an organisaons' own messaging form narraves about humanitarian crises and aid. These narraves have a direct impact
on the "cultures" of help, the relaonships between aid organisaons and their funders, pares to the conict, and host gov-
ernments, and ulmately the ecacy of the response and its accountability to impacted individuals. What inuence do prin-
ciples, beliefs, and interests have on these narraves? Can disnct stories coexist? Who exercises authority over them, and
for what purpose? How do they impact others?
How donor countries support and convey their money will impact the size and shape of the response as well as the capacity
of humanitarian organisaons to handle the aforemenoned dicules. How organisaons solicit and receive private dona-
ons will also have an eect. Donors who direct where and how funds are allocated and promote their humanitarian assis-
tance as part of a package of polical and military support for Ukraine will inuence the atudes of the grant beneciaries.
How may humanitarian giving be reconciled with polical and military objecves? Humanitarian workers (internaonal co-
operaon professionals or volunteers) live within this narrave, which moulds their perspecves and, whether we like it or
not, can be inuenced by the same misinformaon as the general populaon.
For ages, philosophers, theologians, and polical theorists have contested the concept of a "just war" as a contenous and
complicated issue. The view that war is occasionally necessary to ght against aggression, preserve innocent lives, or ad-
vance a just cause is fundamental to the concept of a just war. The conict must be waged for a morally jused purpose,
such as self-defense or the protecon of innocent lives. Except in instances of self-defense or when authorised by the United
Naons Security Council, the United Naons Charter forbids the use of force or the threat of force against the territorial in-
tegrity or polical independence of any state. Thus, the Russian Federaon's invasion of Ukraine is a violaon of internaon-
al law and may result in sancons or other acons by the internaonal community. But, the devil is in the details. In spite of
the majority of UN member states' condemnaon of the invasion, Russia maintains that acted in self-defense because its
naonal security was threatened. In fact, we have all observed, over the past decades, a number of countries successfully
arguing the same concept and jusfying the invasion of a foreign country as an act of self-defense, even when the country in
queson was kilometers away or had an obvious incapacity for real damage. Ulmately, the queson of whether a just war
exists is a maer of perspecve and interpretaon. While some may believe that certain wars meet the criteria for a just
war, others may disagree and argue that all wars are inherently unjust, and that peaceful means should always be used to
resolve conicts.
Humanitarian aid has been subject to intense scruny in recent years. It has been accused of perpetuang conicts by failing
to address their core causes, promote peace, and encourage development. Humanitarian help is many mes thought to fos-
ter dependence on external aid and may not be sustainable over the long run. Most humanitarian workers (who frequently
risk their own lives in the course of their work) are convinced that humanitarian aid is essenal for saving lives and allevi-
Humanitarian News
W A B I P N E W S L E T T E R P A G E 13
ang suering during war and conict. However, most of them also acknowledge that humanitarian aid is frequently insu-
cient to meet the needs of those aected by conict and that aid is merely a bandage for a major wound. And that is be-
cause the tragedy of war is simply unimaginable, it can be sanised so the audience can consume it with their breakfast
news or romancised to generate valour and patriosm where there is only violence, death, disgusng mixtures of blood
and mud, and decaying corpses. Frequently, the most gruesome and horrid parts of bale are those that are not presented
to the public. These unseen tragedies of war serve as a vivid reminder of the devastaon that armed conict can inict on
both individuals and enre society, as well as the urgent need to resolve disputes peacefully.
Yet, this war persists and appears to have a protracted future. The connuance of war is a systemic failure of the polical
and economic structures that govern our planet, which are frequently designed to promote the powerful's interests at the
expense of the many. Elite ambions, movated by the pursuit of prot, resources, and geopolical inuence, frequently
fuel this and any other war. The media and other powerful instuons play a crical role in legimising war as a necessary
evil, while downplaying its horric human costs. In addion, the psychological damage inicted on both military and civilians
adds to a culture of violence and dehumanisaon that diminishes our empathy and compassion. Also, the most vulnerable
and marginalised members of society are disproporonately aected by war's brutality, displacement, and destrucon, as
well as, in this new globalised world, their economic repercussions, even if they reside thousands of kilometres away. The
costs of any bale are borne by regular cizens. To ght the polics of war, we must target the underlying power structures
and work to build a more democrac, fair, and accountable society that priorises the needs and ambions of all individuals
over the narrow interests of the auent and powerful.
It seems not to be in anyone agenda to bring the horrors to an end before they become much worse. Ukraine is uerly dev-
astated, the esmated military fatalies exceeds 250.000, which should be added to the ancipated number of 400.000
severly injured military personnel and probably around 10.000 civilian fatal casuales. More than 13 million people remain
uprooted from their homes, including nearly 8 million refugees across Europe and more than 5 million internally displaced
people within Ukraine, people that probably will not be able to return in a very long me, because their homes, employment
opportunies and living condions no longer exist. Slowly, even ocial voices from "the collecve West" begin to warn that
the quanes of ammunion requested by the Ukrainian government cannot be supplied. The nal outcome of the war does
not appear promising, and it is evident that the connuaon of the conict is not helping Ukranian civilians because of the
terrible suering and death toll it is causing, nor the ordinary cizens of many countries not even ocially involved in the
conict who suer the economic consequences and live in fear of the potenal consequences of the conict's escalaon.
Several naons have eagerly applauded the February 2023 UN General Assembly's demand to embrace the concept that
"Clearly, the world desires peace, and Ukrainians deserve peace. But, not any peace, but just peace ". The problem is that
not every country has a realisc understanding of what a "fair peace" can be at this point in the war. Some may argue for a
return to normalcy. But what would this return to normalcy entail beyond the return of McDonald's, Ikea, and H&M? Does
this imply, for example, that Moscow welcomes Ukraine's membership in the EU and NATO? That the Schengen regime is
extended to the Ukrainian-Russian border? That Ukraine regains control of Crimea and Sevastopol becomes a NATO naval
base? Is this noon of "normality" realiscally possible? Each peace agreement necessitates concessions to make possible to
avoid the perpetuoaon of a war, parcularly when there are evident imbalances in military might. Probably the queson is
how important avoiding war is when the price is paid by a proxy.
If the benets of the perpetuaon of the war can at least be debated, why is it lasng? So, cui bono? Who stands to benet
from this war? In any war, in spite of the widespread destrucon, loss of life, and suering, some individuals and groups may
benet from war. From military contractors to big corporaons including polical leaders and economical elites. But there
is one more collateral gain for the West in this war, an ideological one. Western publics are now vindicated in their self-
delusion that criminal wars are waged only by non-democracies like Pun’s Russia and that there are good, heroic, chival-
rous warriors on one side and evil monsters that are responsible of the only atrocies of the war on the other side. This is
simply not true. The report by the Oce of the High Commissioner for Human Rights (OHCHR) covering the period from 1
August 2022 to 31 January 2023 declares that Russian strikes on crical energy infrastructure since October 2022 have killed
116 civilians and injured 379, causing electricity shortages and damaging medical and educaonal facilies and documenng
the killings of 21 civilians and 214 cases of enforced disappearances and arbitrary detenons by Russian armed forces. But
also stated that Ukrainian armed forces and law enforcement agencies were also responsible for 91 cases of enforced disap-
pearances and arbitrary detenons. OHCHR interviewed eight individuals prosecuted for "collaboraon acvity" and docu-
Humanitarian News
W A B I P N E W S L E T T E R P A G E 14
mented the arbitrary detenon of 88 Russian civilian sailors. War is (and has always been) a brutal and deshumanizing
force and not an exercise of chivalry. However, aer many years of ethical instability, or in Artemy Magun's terms, ethical
negavity, this war supports the illusion that good and evil are disnct, all signicant polical subjects are ethically marked
as heroes or as villains, and, most importantly, the self-idencaon of individuals as ethical subjects has acquired a total
and universal character. Act in such a way that the Kanan maxim of your will can be acknowledged as a universal law. But
probably, that is just a delusional phantasy, hard to sustain in a moment when the legimacy of opinion leaders, mainstream
media, government instuons, and naonal or internaonal legal bodies is severely cricised by a huge poron of society
Everybody should keep in mind that persisng on its present course, the war will come to vindicate the view of much of the
world outside the West that this is a U.S.-Russian war with Ukrainian bodies — increasingly corpses. Not even a well-
funconing doctrinal system in which “unpopular ideas can be silenced, and inconvenient facts kept dark, without the need
for any ocial ban,” (to borrow George Orwell’s descripon of free England in his introducon to Animal Farm) will prevent
that.
Do opportunies for diplomacy sll remain? As ghng connues, posions predictably harden. Right now, Ukrainian and
Russian stands appear irreconcilable. That is not a novel situaon in world aairs. It has oen turned out that “Peace talks
are possible if there is a polical will to engage in them". However, if the only available language is mutual vilicaon and
demonizaon, oen accompanied by grandiose rhetoric about the cosmic struggle between the forces of light and darkness
and for prioritazion of geopolical interests and imposion of one's own worldview, the chances of a just and realisc peace
will remain remote.
As educated cizens we have a responsibility to give our own informed opinions on all the important topics that impact on
our sociees, because our opinions carry weight and can inuence others. We have a responsibility to enhance democracy,
and for a democracy to funcon, individuals must be well-informed and free to express their opinions. We may contribute to
the promoon of crical thinking by encouraging others to engage in logical debates and crical thought, and by combang
disinformaon. Indierence is an unaainable luxury. We, who have the advantage of a higher educaon, are the ones who
must consult mulple sources to gain a comprehensive understanding of what is occurring, who must examine the evidence
to support both sides of the argument, and who must avoid conrmaon bias by avoiding looking at the informaon in a
way that conrms our preconceived noons. If we wish to live in a democracy, we must have the parcipaon of a crical
mass of cizens who do not follow or give credence to popular opinion or just repeat what is told by the mainstream media,
but instead coin and communicate their own opinions and demand accountability from policymakers.
And as regular cizens, we must acknowledge that war is not a soluon, but rather a symptom of more fundamental social
and polical issues that require innovave and compassionate answers. We can only hope to create a more just and peace-
ful society for ourselves and future generaons if we culvate a spirit of cooperaon, understanding, and mutual respect,
whichever our ideological dierences. By working together and taking responsibility for our collecve future, we can create a
society that is more equitable and sustainable for everyone. Otherwise, any humanitarian aid will be a charade, a palliave
for the real needs of the suering, and a sedave for our consciences.
Polarisaon is characterisc of the current era, and many readers will disagree with these opinions. These are the sen-
ments of someone who has spent the last three decades sloshing through enough mud, dragging too many corpses, and wit-
nessing too many atrocies. And who believes that if we are unable to discover a major transformaon in how we manage
naonal and internaonal dierences, Hell will remain empty because all the devils will remain here.
*The views expressed in this arcle are those of the author (Silvia Quadrelli) and do not necessarily reect the ocial posi-
ons of the Execuve Board or Internaonal Board of Regents of the WABIP.
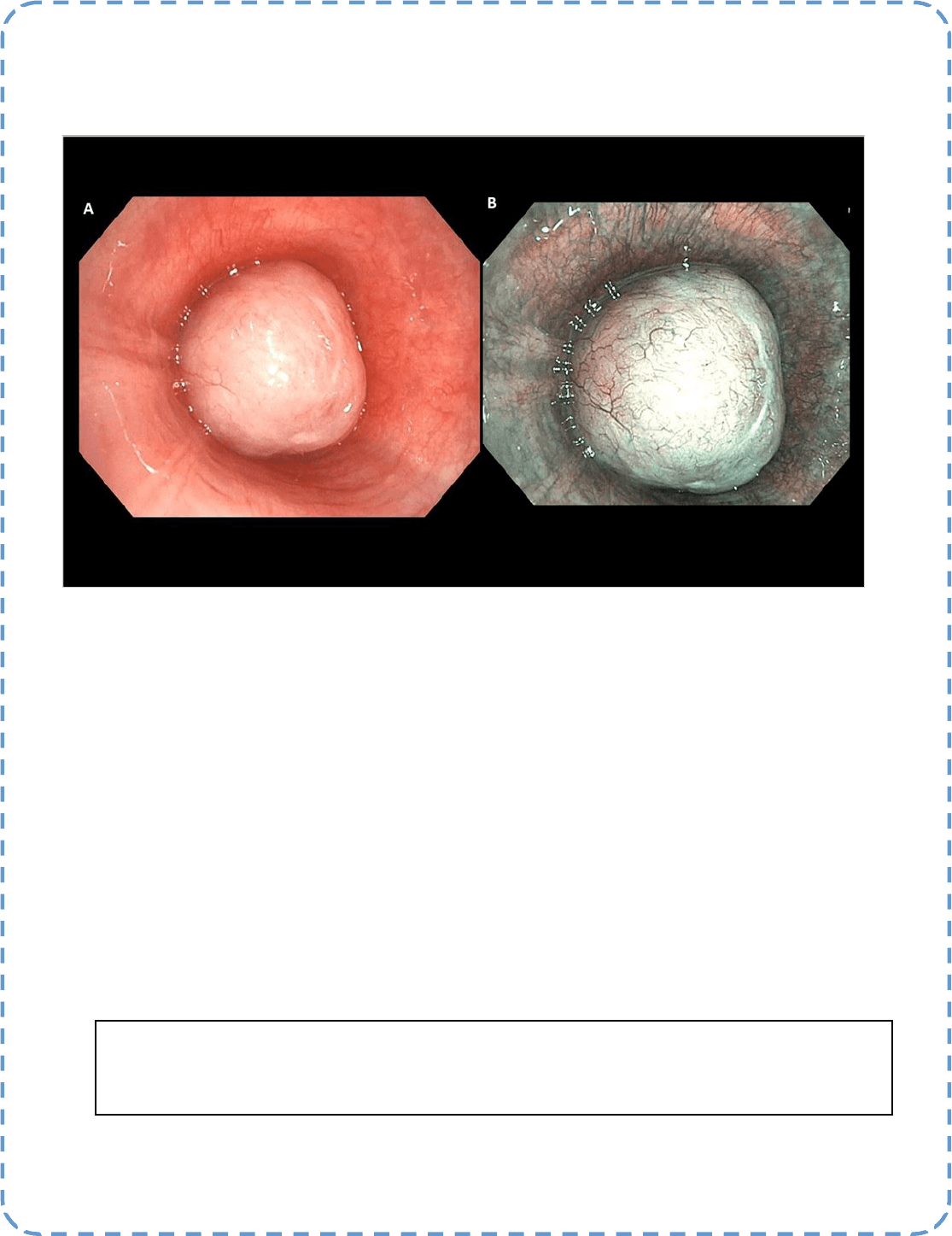
Best Image Contest 2023 (2 of 3)
Descripon: Endobronchial Leiomyoma of the Le Main Bronchus
A. White Light Image
B. Narrow Band Image
Submier(s): Hari Kishan Gonuguntla, Pree Vidyasagar, Aravind Ram
Best Image Contest
P A G E 15
This image is 1 of 3 selected among 100+ submissions to our Best Image Contest held in late 2022. Our next
Image Contest will open later this year. We look forward to receiving your image submissions.
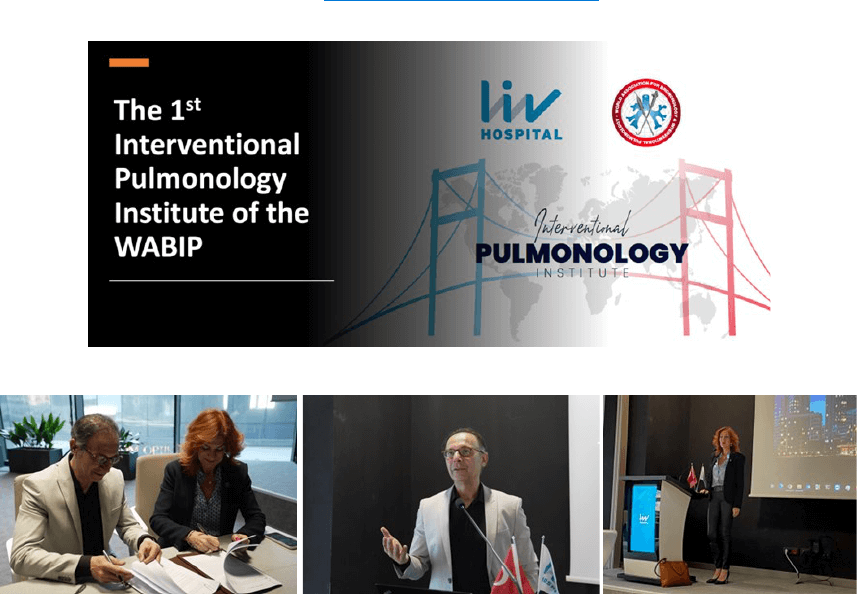
P A G E 16
WABIP News
The 1
st
Intervenonal Pulmonology Instute (IPI)
of the WABIP Inaugurated in Istanbul, Turkiye
hps://www.wabip.com/instute
On Sunday, April 30th, 2023, during a beauful ceremony in Istanbul, the leaderships of the World Associaon for
Bronchology and Intervenonal Pulmonology (WABIP) and the LIV hospital, Istanbul (Vadistanbul) signed the rst-of-its
-kind agreement to inaugurate the rst Intervenonal Pulmonology Instute (IPI). This remarkable contract between a
non-prot conglomerate of more than 50 naonal intervenonal pulmonology sociees (WABIP) and a private hospital
chain in Istanbul Turkiye was signed by Meri İsro, CEO of LIV hospital system, and Dr. Ali Musani, chairman of the 1st
Intervenonal Pulmonology Instute. This collaboraon starts a new chapter in medical teaching and training of doc-
tors from developing countries by the hundreds of IP faculty from dozens of countries worldwide to disseminate sci-
ence and skills of IP without geographical or polical restricons.
The ceremony was followed by the rst IPI conference, where Dr. Musani presented the mission, vision, organizaonal
structure, educaonal goals, and details of the partnership between the two organizaons. He outlined the short-term
and long-term plans of the IPI and introduced the dierent commiees, including the fellowship selecon commiee,
educaon/curriculum commiee, and IPI commiee. He emphasized that IPI’s fundamental goal is to train pul-
monologists from the developing parts of the world in IP, free of charge, so they can go back and serve their countries
and educate/train others in the IP eld. Soon aer the ceremony and introductory speeches from Meri İsro and Dr.
Musani, the academic poron of the conference started.
Meri İsro, CEO of the LIV hospital system, and Dr. Ali Musani, chair of the Intervenonal Pulmonology Instute, signed the
landmark contract between the two instuons before outlining their visions in front of the audience

P A G E 17
WABIP News
The front desk of the LIV Hospital, Vadistanbul Turkiye
The conference had several internaonal speakers from Europe and the USA represenng the WABIP. Aendees from
dierent parts of Turkiye parcipated in the conference and brought complex IP cases to seek expert opinions from the in-
ternaonal faculty.
IPI faculty and aendees at the rst IPI conference on 4/30/2023 in Istanbul, Turkiye
P A G E 18
WABIP News
Dr. Levent Dalar, Director IPI Istanbul
FELLOWSHIP:
This day also marks the ocial announcement of the beginning of the IP fellowship at the IPI.
Pulmonologists and thoracic surgeons worldwide are welcome to apply for the WABIP-IPI Intervenonal Pulmonology (IP) fellowship
starng Oct 1st, 2023. Please review the details of the IP fellowship requirements and curriculum (hps://www.wabip.com/instute)
before applying for the fellowship. Please ll out the applicaon forms available at hps://www.wabip.com/instute and send them to
Dr. Javier Flandes, chair of the fellowship selecon commiee (jandes@quironsalud.es), and Dr. Levent Dalar, director for the IPI Istan-
bul (leventdalar@gmail.com ) at least four months before the start date of the fellowship. Please see below for the fellowship applica-
on deadline.
Applicaon Deadlines:
The selecon commiee will respond to your applicaon in three weeks to allow you ample me to nalize your travel preparaons.
The IPI will happily provide you with a leer of acceptance to help you obtain a Turkish visa. You should not engage in any employment
or illegal acvies in Turkiye. IPI will fully cooperate with the legal authories in providing informaon regarding you if asked. IPI does
not pay salaries or any nancial support to trainees and fellows. You should not expect any nancial support from IPI or the LIV hospital.
EDUCATION AND TRAINING:
The fellowship will be three months long, starng Oct 1st, 2023. As outlined above, one or two new fellows will start every three
months. The fellows will be required to stay in Istanbul for three months and work with the local and internaonal vising faculty of the
WABIP. They will be provided with limited malpracce coverage by the LIV hospital and a temporary trainee license from Isnye Univer-
sity, Istanbul, to perform procedures under the supervision of the local IP faculty. The fellows will be expected to work six days a week,
including Saturday, and go to other hospitals with the IP faculty to perform procedures.
Fellowship Start Date Applicaon Deadline
The applicaon and supporng material should be
received by
Oct 1
st
July 1
st
Jan 1
st
September 1
st
April 1
st
December 1
st
July 1
st
March 1
st
P A G E 19
WABIP News
IPI will provide a reading list, a library of procedural videos, and review material. We expect every fellow to study all the pre-fellowship training
material prior to starng the fellowship. All fellows will undergo pretesng in theory and skills of IP procedures. The purpose of the pretest is
to gauge their improvement aer the fellowship with a posest/cercaon test. The pretest will not be used to select or reject candidates
from the fellowship.
If your budget allows, we would like you to travel to Athens, Greece, Florence, Italy, or Ancona, Italy, for a week of free simulaon training with
high-delity simulators and cadavers under WABIP faculty. This training is not mandatory but will help you get comfortable with more complex
procedures, such as rigid bronchoscopy, airway stenng, etc. We plan to do this training in the early weeks of each fellowship period.
IPI Faculty
FEE and EXPENSES:
The IPI will not charge any fee for training fellows, but the fellows will be responsible for all their expenses, including ights, stay for three
months in Istanbul, and food during their fellowship. WABIP is trying to raise funds with donaons and scholarships to support a few fellows
yearly, but we don’t expect any support for at least one year. We encourage fellows to obtain health insurance in Turkey to avoid unnecessary
charges if they get sick while training in Istanbul. IPI does not pay trainees and fellows. You should not expect any nancial support from IPI.
We encourage you to seek support from your respecve governments, hospitals, industry grants, scholarships, etc. We will gladly furnish sup-
porng documents to help you obtain these grants if needed.
VISA:
IPI will help you obtain a visa by providing a leer of acceptance by the WABIP-IPI Istanbul. You are expected to apply for the visa at least three
months in advance so that in case of your inability to obtain a visa in a mely fashion, we can oer the fellowship spot to other candidates. We
expect you to have your visa and ckets ready and emailed to the selecon commiee at least three months before your fellowship start date.
Cercaon:
Each fellow will be tested during the last week of their three months of training. This test will comprise of didacc and skills tesng. Please see
the skills tesng document. You will be trained in skills and steps of IP procedures the same way as you will be tested. Each fellow must pass
both didacc and skills test to obtain the cercate of compleon of the IP fellowship at the WABIP-IPI. This cercate does not give you a
license to pracce IP/bronchoscopic and pleural procedures at your instute, in your country, or in any other country. To pracce these proce-
dures, you must sll fulll your country's and instuon's requirements, such as local credenaling and licensing. Due to a relavely short
training period, we cannot guarantee that you will be fully competent in your skills to perform IP procedures independently aer just three
months of training. The required number of procedures for IPI training is reduced substanally to allow you to nish the training in three
months.
P A G E 20
WABIP News
You will be more than welcome to apply for the same fellowship again to obtain more experience. You must undergo
the same selecon process as the rst me. You should do some supervised procedures at your home intuion to be
comfortable doing them and fulll your naonal and instuonal credenaling and licensing requirements. We strongly
recommend some supervised training before performing IP procedures independently. We also strongly recommend at
least 1-2 years of pracce with four mes, or a greater number of procedures done/required during the IPI fellowship
before teaching others in your country or starng a formal training program. We will try to organize a symposium for
all the IPI fellows at the World Congress of Bronchology and Intervenonal Pulmonology (WCBIP) every other year.
WABIP-IPI will gladly stay in touch with all its graduates and provide connued educaon and guidance.
Code of Conduct:
The fellows will be required to follow the code of conduct of the LIV hospital in their day-to-day work and social inter-
acons while training there. The fellows must follow the hospital's and IP program's rules and policies. The IPI director
and the chair reserve the right to expel any fellow who misbehaves and does not follow the rules and regulaons of the
instuon or is disrespecul and disrupve. In case of expulsion from the program, the fellow must return to their
home country within two weeks, and they will be deemed incompetent to receive IPI cercaon. IPI also reserves the
right to inform immigraon authories of any illegal acvies and take legal acon if any criminal acvity is suspected.
IPI fellows are supposed to refrain from engaging in any employment while in Turkiye for training at the IPI. They will
be reported to immigraon if any such acvity is brought to IPI's aenon.
In conclusion, IPI training will give you a strong foundaon to build your IP career. Our faculty of world experts have
developed a robust training program to train you in as many skills as possible in a short me. We will stay engaged with
you long aer your fellowship to provide you with mentors, educaonal opportunies, and advice when asked to make
sure that you have all the professional and moral support you need to start a successful program in your home country
and educate the next generaon of doctors and connue the mission of elevang the level of health care in your coun-
try.
Sincerely,
The Intervenonal Pulmonology Instute Commiee of the WABIP
hps://www.wabip.com/instute
P A G E 21
Education
WABIP Workshop in Buenos Aires March 2023
The World Associaon of Bronchology and Intervenonal Pulmonology (WABIP) recently hosted the 3rd Bronchoscopy Course-
Workshop in Buenos Aires, Argenna. Aended by 35 respiratory medicine professionals from Argenna and neighboring coun-
tries, the workshop catered to individuals with intermediate or advanced levels of prior bronchology training who are acvely
working in bronchoscopy.
The course and workshop were led by renowned internaonal expert Dr. Sara Tomasse from Italy, alongside highly experi-
enced local instructors Artemio Garcia, Silvia Quadrelli, Patricia Vujacich, Hugo Boo, Marcos Las Heras, and Jose Rodríguez Jimé-
nez from Argenna, as well as David Lazo from Chile. Aer a day of informave lectures, parcipants enjoyed a full day of hands-
on training at various staons, covering reusable bronchoscopes, rigid bronchoscopy, cryotechniques, stenng, EBUS, dicult
tracheal intubaon, and laser.
Under the watchful guidance of the course instructors, each parcipant had the chance to pracce each technique using a di-
verse array of inanimate models. This learner-centered educaonal experience maintained a low student-teacher rao, allowing
local and internaonal experts to oer more personalized aenon to each student. Instructors were able to assess individual
strengths, weaknesses, and learning styles, tailoring their teaching methods to meet specic needs and providing customized
feedback for improvement. The local team skillfully organized the two-day program, resulng in a memorable and enriching ex-
perience for all. The unusual hot weather in Buenos Aires prompted the selecon of a beauful locaon in the Delta islands,
where parcipants could appreciate nature and forge friendships. Aendees greatly valued the opportunity to network with WA-
BIP professionals in an environment that fostered camaraderie, curiosity, and passion.
WABIP would like to extend its gratude to the bronchoscopy training instructors and the organizing team for their commitment
to expanding global bronchoscopy training. The ulmate goal is to develop procedures that are not only safer and more reliable
but also completely comfortable for all paents, regardless of their geographic locaon. The exceponal vising educator, Dr.
Sara Tomasse, played a crucial role in the event, and her contribuons were greatly appreciated by all parcipants.
Can You Smell Cancer?
Stracaon of lung nodules is indeed the bane of lung cancer screening and early diagnosis. Even in the meculously selected paents in the Na-
onal Lung Cancer Screening Trial (NLST), more than 95% of the paents diagnosed with pulmonary nodules were benign aer surgical resecon.
Our quest for accurately idenfying high-risk pulmonary nodules goes on. We have gained some ground with PET scans, proteomics, and genomics,
but we sll need to achieve desired precision and eciency (less invasive and accurate). Although our technological advances in accurately sam-
pling pulmonary nodules with state-of-the-art robocs, ancillary technologies, cone beam CT scanners, and the like have evolved rapidly, we sll
biopsy more benign nodules than we should. Our struggle for more precise idencaon of malignant nodules goes on.
Exhaled breath contains a gas mixture of volale organic compounds (VOCs) that result from ssue metabolism. In unique physiologic and patho-
logical condions, the VOCs dier in their composions. The analysis of VOCs in dierent condions to understand and diagnose physiologic and
pathological states has been of great interest over the decades. For a long me, recognizing specic paerns or signatures of VOCs in dierent con-
dions with reasonable accuracy has been the research topic. Gas chromatography-mass spectrometry and mimicking olfacon with mechanical
noses have shown promise in diagnosing cancer in early work.
Exhaled breath analysis of VOCs in lung cancer has been studied for quite some me, but validaon studies and clinical implementaon sll need
to be improved. Recently, a very interesng publicaon in CHEST 2023 from the Netherlands showed promising results in diagnosing non-small cell
lung cancer (NSCLC) by exhaled breath proling using an electronic nose. The study from Kort et al. (1) looks at two important quesons; 1, can a
predicon model be validated to disnguish non-small cell lung cancer paents from paents without non-small cell cancer 2, would adding this
test to other clinical informaon available will improve lung cancer diagnosis?
Five-minute normal breathing into a handheld electronic nose (aeoNose) test was performed on 376 subjects in a mulcenter study in the Nether-
lands. The trial resulted in a 95% sensivity and 51% specicity and a negave predicve value of 94%. The study suggests that combining clinical
informaon with exhaled breath data can disnguish paents with non-small cell cancer from subjects without non-small cell lung cancer in a non-
invasive manner.
Editor-in-Chief: Dr. Kazuhiro Yasufuku
Research
Primary Business Address:
Kazuhiro Yasufuku, Editor-in-Chief WABIP
Newsleer
c/o Judy McConnell
200 Elizabeth St, 9N-957
Toronto, ON M5G 2C4 Canada
E-mail: newsleer@wabip.com
P A G E 22
Associate editor:
Dr. Ali Musani
Associate editor:
Dr. Sepmiu Murgu
Ali I. Musani MD, FCCP
University of Colorado School of Medicine,
Denver
Mulple studies in the past have alluded to similar outcomes in dierent study designs and cohorts. The study from Kort et al. (1) showed
signicant improvement in the predicon of NSCLC when breath analysis of VOC was added to clinical informaon commonly used in other
predicon models for lung cancer. Using newer predicve models with VOC analysis in high-risk paents with pulmonary nodules and clinical
data, CT, and PET scans could make lung nodule stracaon more precise.
Due to its simplicity and non-invasive applicaon, this test can be used as a “point-of-care” test that can be easily implemented in the early
diagnosis of lung cancer (lung nodule clinics or lung cancer screening programs) in an outpaent seng.
Reference:
1. Kort S. Chest. 2023 Mar;163(3):697-706.
Research
P A G E 23
P A G E
24
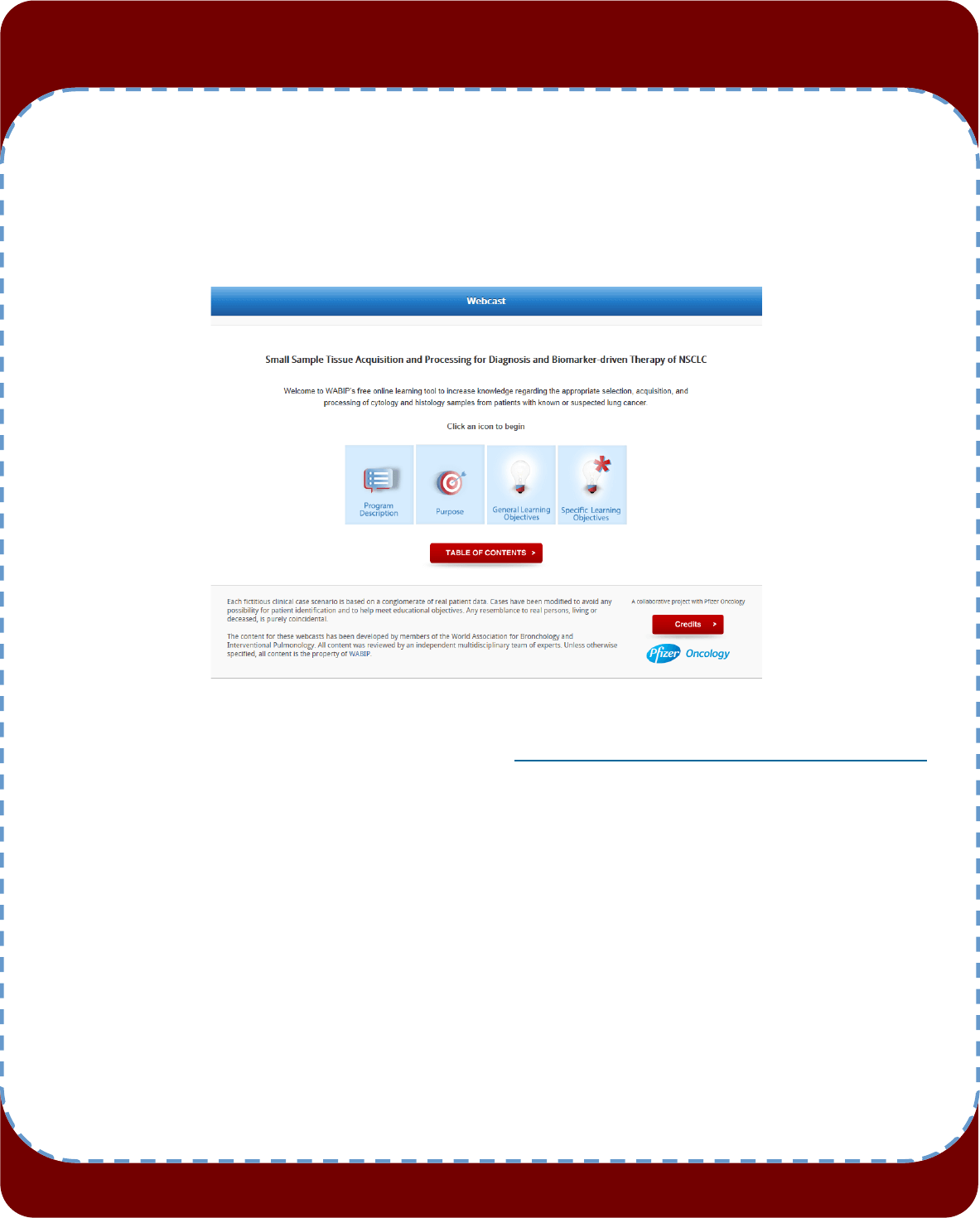
WABIP ACADEMY- WEBCASTS
The WABIP has started a new educaon project recently: THE WABIP ACADEMY. The WABIP Academy will pro-
vide free online webcasts with new and hot topics that will interest pulmonologists and intervenonalists.
Current webcast topic: Tissue acquision for biomarker directed therapy of NSCLC
You can reach these webcasts by using this link: hp://www.wabipacademy.com/webcast/
www.bronchology.com Home of the Journal of Bronchology
www.bronchoscopy.org Internaonal educaonal website for
bronchoscopy training with u-tube and
facebook interfaces, numerous teachiing
videos, and step by step tesng and assess
ment tools
www.aabronchology.org American Associaon for Bronchology and I
ntervenonal Pulmonology (AABIP)
www.eabip.org European Associaon for Bronchology and
Intervenonal Pulmonology
W A B I P N E W S L E T T E R
Links
www.chestnet.org Intervenonal Chest/Diagnosc Procedures (IC/DP)
NetWork
www.thoracic.org American Thoracic Society
www.ctsnet.org The leading online resource of educaonal and
scienc research informaon for cardiothoracic
surgeons.
www.jrs.or.jp The Japanese Respirology Society
sites.google.com/site/asendoscopiarespiratoria/
Asociación Sudamericana de Endoscopía Respiratoria
P A G E 24