Volume 12
Issue 01
JANUARY 2024
Inside This Issue
Editorial, 2-3
Technology Corner, 4-9
Tips from the Experts, 10-12
Humanitarian News, 13-18
Best Image Contest, 19
WABIP News, 20
Research, 21-22
Links, 23
Up and-coming Bronchoscopic Ablation Therapies for
Treatment of Lung Cancer
WABIP Newsletter
J A N U A R Y 2 0 2 4 V O L U M E 1 2 , I S S U E 1
EXECUTIVE BOARD
Stefano Gasparini, MD
Italy, Chair
Pyng Lee, MD, PhD
Singapore, Vice-Chair
Hideo Saka, MD
Japan , Immediate Past-
Chair
Silvia Quadrelli, MD
Membership Commiee
Chair
Jean-Michel Vergnon, MD
Educaon Commiee
Chair
Ali Musani, MD
Finance Commiee Chair
Naofumi Shinagawa, MD
Japan,
Secretary General
Menaldi Rasmin, MD, PhD
Indonesia , President
WCBIP 2024
Rajesh Thomas, MD, PhD
Melbourne , President
WCBIP 2026
STAFF
Michael Mendoza
General Manager
Judy McConnell
Administrator
Kazuhiro Yasufuku
Newsleer Editor-in-chief
P A G E 2
Stereotacc beam radiaon therapy (SBRT) has tra-
dionally been the standard of care for paents with
early-stage lung cancer and thoracic oligometastac
disease who are not surgical candidates. SBRT has
been dened as large doses of radiaon ( > 6 Gy/
fracon) administered over a few (<=5) fracons
1
.
This administraon of large doses of radiaon can
be associated with signicant toxicies both to the
treatment sites and the adjacent normal structures
that can become collateral damage. Complicaons
include pneumonia, pneumonis, chest wall pain, rib
fractures, brachial plexus injury, etc.
2
3
The risk of
complicaons seems to be higher for more central
and ‘ultra’ central tumors as they are situated closer
to the crical thoracic structures
4
. Similarly, paents
with pre-exisng intersal lung diseases are at a
higher risk of pneumonis as well, with some studies
reporng a risk of fatal radiaon pneumonis at 6%
5
.
Given the above limitaons, there has been a signi-
cant interest in developing minimally invasive abla-
ve technologies that can be administered via trans-
bronchial or image-guided transthoracic routes.
These modalies include radiofrequency ablaon
(RFA), microwave ablaon (MWA), cryoablaon, and
more recently pulsed electric eld (PEF) systems.
RFA involves placing a probe into the lesion, through
which alternang current is passed. This produces
heat and can generate a temperature of > 100◦C in
the vicinity of the target with resultant necrosis of the le-
sion
6
7
. However, as the lesion is charred, it impedes the
conductance of current and heat, which may limit the abla-
on zone. Similarly, blood owing through any adjacent
vessels acts as a ‘heat sink’, thereby making it harder to
reach the intended target temperature and therefore lim-
ing the ablaon ecacy and zone. MWA which uses alter-
nang electromagnec waves to oscillate water molecules
and generate friconal heat, is more resistant to these limi-
taons and therefore can potenally achieve higher tem-
perature and a larger ablaon zone
6
. Pneumothoraces and
bleeding are the most signicant complicaons for MWA
8
9
.
Tumor cryoablaon involves introducing a cryoprobe into
the lesion; mulple freeze-thaw cycles are then used to
induce cell death. Like most image-guided transthoracic
ablave modalies, the most frequent complicaon is
pneumothorax; however, more serious complicaons such
as hemopneumothorax and hemoptysis have also been
reported
10
.
The newest ablaon modality is the pulsed electric eld
(PEF) therapy. Unlike the aforemenoned therapies, it
doesn’t rely on heat or cold to degenerate tumors; rather, it
uses brief high voltage current to alter the cell membrane
potenals, thereby interfering with normal cell homeostasis
and eventually leading the cell death f
11
12
. As a result, the
extracellular matrix is preserved. Furthermore, angens are
released from the tumor, which may induce an an-tumor
immune response as well. The fact that extracellular matrix
and lymphac drainage are preserved, together with the
Muhammad Sajawal Ali MD
Assistant Professor of Medicine,
Weill Cornell Medicine,
New York, NY
Ali Musani MD
Professor of Medicine and Surgery,
University of Colorado School of
Medicine, Denver
W A B I P N E W S L E T T E R
P A G E 3
References:
1. Poers L et al. Int J Radiat Oncol Biol Phys. 2010;76(2):326–332.
2. Andolino DL et al. Int J Radiat Oncol Biol Phys. 2011;80(3):692–
697.
3. Forquer JA et al. Radiother Oncol. 2009;93(3):408–413.
4. Lindberg K et al. J Thorac Oncol. 2021;16(7):1200–1210.
5. Onishi H et al. Cancers (Basel). 2018;10(8):257.
6. Bartle EC et al. Lung Cancer 2023;176:14–23.
7. Zhong C-H et al. European Respiratory Journal [Internet] 2023
[cited 2024 Jan 3];62(suppl 67). Available from: hps://
erj.ersjournals.com/content/62/suppl_67/OA2598
8. Tran S et al. European Respiratory Journal [Internet] 2017
[cited 2024 Jan 3];50(suppl 61). Available from: hps://
erj.ersjournals.com/content/50/suppl_61/PA4282
9. Lau KKW et al. J Bronchology Interv Pulmonol. 2023 Sep 25. doi:
10.1097/LBR.0000000000000950.
10. Zhang Y-S et al. J Thorac Dis. 2016;8(Suppl 9):S705–S709.
11. Wagsta PG et al.. Onco Targets Ther. 2016;9:2437–2446.
12. Irreversible electroporaon of lung neoplasm: A case series -
PMC [Internet]. [cited 2024 Jan 3];Available from: hps://
www.ncbi.nlm.nih.gov/pmc/arcles/PMC3560719/
13. Galvanize Therapeucs, Inc. The Galvanize Therapeucs Early
Stage, Non-Small Cell Lung Cancer, Treat and Resect Study
[Internet]. clinicaltrials.gov; 2023 [cited 2023 Dec 31]. Available
from: hps://clinicaltrials.gov/study/NCT04732520
14. Inc GT. Galvanize Therapeucs Announces Promising Data on
the Aliya
TM
Pulsed Electric Field (PEF) System in Early-Stage Non-
Small Cell Lung Cancer [Internet]. [cited 2024 Jan 3];Available
from: hps://www.prnewswire.com/news-releases/galvanize-
therapeucs-announces-promising-data-on-the-aliya-pulsed-
electric-eld-pef-system-in-early-stage-non-small-cell-lung-cancer
-301977976.html
15. Inc GT. Galvanize Therapeucs Begins U.S. Clinical Study Using
Aliya
TM
Pulsed Electric Field (PEF) for Stage IV Non-Small Cell Lung
Cancer or Metastasis to the Lung [Internet]. [cited 2024 Jan
3];Available from: hps://www.prnewswire.com/news-releases/
galvanize-therapeucs-begins-us-clinical-study-using-aliya-pulsed
-electric-eld-pef-for-stage-iv-non-small-cell-lung-cancer-or-
metastasis-to-the-lung-301932837.html
fact that a capsule of scar ssue doesn’t form, can
potenally further enhance the immune response.
The an-tumor eect is achieved via both direct
ablaon and indirect immune response. The an-
tumor immune response can be observed at distal
tumor sites as well. INCITE-ES is an internaonal
treat and resect study for early-stage non-small cell
lung cancers to assess the safety and immune ac-
vaon
13
. Early results suggest PEF therapy induces
a strong immune response in the tumors
14
. AFFINI-
TY is another major mulcenter prospecve study
assessing the safety and eecveness of PEF thera-
py in paents with metastac pulmonary lesions
15
.
In summary, while the data is sll limited on the
safety, ecacy, and technical parameters for lung
cancer ablave therapies, mulple modalies ap-
pear promising. There is signicant excitement
around PEF therapy, since in addion to local abla-
on it may increase the ecacy of immunotherapy
both locally and at distant sites. These therapies
can be administered both via transthoracic and
bronchoscopic routes. Therefore, it would be feasi-
ble to potenally oer a tumor biopsy and therapy
in the same seng. Further studies are needed
before these ablave therapies can be rounely
adopted. However, they are well and truly on the
way to becoming alternaves and, in some cases,
even replacing SBRT and surgery.
W A B I P N E W S L E T T E R
P A G E 4
Technology Corner
Tracheostomy Tubes: Types and their Pros and Cons
Introducon
Tracheostomy, a surgical procedure involving the creaon of an opening in the anterior wall of the trachea, is an intervenon per-
formed by many specialists (ENT, Intervenonal Pulmonology, Trauma, Crical Care, Thoracic Surgery) in a variety of urgent and non
-urgent scenarios. It establishes a secure airway in paents who can’t be intubated translaryngeally and facilitates transion of care
and potenally weaning o the venlator in crically ill paents who require prolonged respiratory support. Central to this proce-
dure is the tracheostomy tube, a device that maintains the patency of the tracheostomy stoma and airway patency. In this essay, we
explore the diverse types of tracheostomy tubes, discussing their features and clinical applicaons.
Background
Tracheostomy tubes have evolved over the years to meet the specic needs of paents across a spectrum of medical and surgical
condions. The basic design involves a tube inserted into the tracheostomy stoma to secure a patent airway. The materials, shape,
and addional features of these tubes vary, catering to the unique requirements of paents with dierent condions. Knowing the
indicaons and potenal problems of specic tracheostomy tubes is relevant for healthcare providers performing the procedure and
caring for paents with indwelling tracheostomy tubes.
Clinical Indicaons
Common indicaons include acute upper airway obstrucon, post-cricothyrotomy cases, facial/neck fractures, penetrang laryngeal
trauma, need for prolonged mechanical venlaon, compromised airway protecon (inability to clear secreons despite maximal
noninvasive measures), refractory sleep apnea/obesity hypovenlaon syndrome, special cases of subgloc stenosis (inoperable
and recurrent aer mulple endoscopic procedures and not amenable to stenng), severe vocal cord paralysis, burns or inhalaon
injuries, and anatomic abnormalies altering upper airway structure. In our pracce, primary use involves venlator weaning for
crically ill paents with acute respiratory failure or neurologic disorders requiring prolonged venlatory support.
Sepmiu Murgu, MD, FCCP, DAABIP
Department of Medicine,
Division of Pulmonary and Crical Care
The University of Chicago
Prince Namoah, MD
Department of Medicine,
Division of Pulmonary and Crical Care
The University of Chicago
W A B I P N E W S L E T T E R
P A G E 5
Types of Tracheostomy Tubes: Features and Clinical Ulizaon
Tracheostomy tubes come in various types from several manufacturers, each designed to address specic clinical needs (Table 1).
The dimensions of tracheostomy tubes are given by their inner diameter, outer diameter, length, and curvature (degree of angula-
on). Dierences in dimensions between tubes with the same inner diameter from dierent manufacturers may have important clini-
cal implicaons, depending on the other features.
Diameter: If the inner diameter is too small, it will increase the airow resistance through the tube and make the airway clearance
more dicult. Larger outer diameter tubes will be more dicult to pass through the stoma and could result in carlage fracture and
subsequent stenosis or malacia.
1–3
If the outer diameter is too large, the leak with the cu deated will be decreased, and this will
negavely impact the ability to use the upper airway with cu deaon for speech prior to the tracheostomy tube exchange (when
possible). Smaller outer diameter tubes, on the other hand, may require increases in the cu pressure needed to avoid signicant
cu leak and high pressures could eventually lead to stenosis at the level of the cu.
4
Length: If the tracheostomy tube is too short, the distal end can get obstructed against the posterior tracheal wall, or even against
the anterior wall if the inseron site is high (due to tube angulaon). This can be remedied by using a larger tube, a tube with a dier-
ent angle (see Table), a tube with a more exible sha, or a tube with extra length. Extra length tubes are constructed with extra
proximal length (vercal extra length) or with extra distal length (horizonal extra length) (Figure). Extra proximal length facilitates
tracheostomy tube placement in paents with a large neck circumference, which can be measured by bedside ultrasound or neck
computed tomography, when available. Extra distal length facilitates placement in paents with tracheal stenosis, tracheomalacia or
tracheal anomalies that need to be bypassed or, as in our pracce, in certain paents, to assure a more proper alignment of the tube
with the tracheal lumen axis. Care must be taken to avoid inappropriate use of these tubes because they may even cause carinal
trauma if too long or induce distal tracheal stenosis if the cu is inadvertently overinated.
Cu: Tracheostomy tubes can be cued or uncued. Uncued tubes allow airway clearance but provide no protecon from aspira-
on and cannot usually be used for venlaon if paents need venlatory support. Cued tracheostomy tubes allow secreon clear-
ance and oer some protecon from aspiraon, and posive pressure venlaon can be more eecvely applied when the cu is
inated. Specic types of cus used on tracheostomy tubes include high-volume low-pressure cus, ght-to-sha cus (low-volume
high-pressure), low volume-low pressure cus and foam cus (Table). High-volume low-pressure cus are most used and maintaining
opmal tracheal cu pressure is crucial for paent safety. The normal tracheal capillary perfusion pressure is 25–35 mm Hg. Cu
pressure should be kept at 20–30 cm H
2
O (15–22 mm Hg) and monitored every shi to minimize risks of tracheal injury (when too
high) and aspiraon (when too low). Regular monitoring, especially during tube changes or posion adjustments, is recommended
but in pracce this is extremely dicult to achieve and in fact, in a study, underinaon (pressure < 20 cm H
2
O) was noted in 54% of
paents, and overinaon (pressure > 30 cm H
2
O) occurred in 73% of paents.
5
Two cu types, the low volume, high pressure and
foam cu, serve dierent purposes. The former minimizes airow obstrucon outside of the tube when the cu is deated and is
intended for paents requiring intermient cu inaon. The foam cu consists of a large-diameter high residual volume cu com-
posed of polyurethane foam. It was designed to address the issues of high lateral tracheal wall pressures, that lead to complicaons
W A B I P N E W S L E T T E R
P A G E 6
such as tracheal necrosis and stenosis (Figure). Despite its advantages, the foam cu is not widely used, typically reserved for paents
with exisng tracheal injuries. Regular cu deaon is advised to check integrity and prevent adhesion to the tracheal mucosa.
The newer model of low pressure, low volume cus have a tapered shaped (Taper Guard) cu (Figure), and in experimental models
has less lateral wall pressure and larger inner diameter facilitang increased airow around the outer cannula (when cu deated).
There are reports of increased cu leak with these tubes as the tapered cu design may t dierently in paent’s airways over me
but this could also be due to decreased airway edema or a component of tracheomalacia at tracheostomy cu site
6
Adjustable tubes: Several tube designs have a spiral wire-reinforced exible design (See Bivona tube, Figure). These tubes are not
compable with lasers, electrosurgical devices, or magnec resonance imaging. Some have a moveable ange designed to allow ad-
justments to beer t the tube to the paent’s unique anatomy. Because the locking mechanism on the ange tends to deteriorate
over me, these tubes should be considered a temporary soluon. For long term use, the adjustable ange tube should be replaced
with a tube that has a xed ange. Custom-constructed tubes are available from several manufacturers to meet this need.
Inner cannula: Some tracheostomy tubes are used with an inner cannula known as dual-cannula tracheostomy tubes. In some cases,
the venlator adaptor is on the inner cannula, and the venlator cannot be aached unless the inner cannula is in place. The use of
the inner cannula allows it to be cleaned or replaced at regular intervals without removing the tracheostomy tube from its stoma.
The inner cannula can be removed to restore patent airway if the tube occludes, which may be an advantage for long term use out-
side an acute care facility. One potenal issue with the use of an inner cannula is that it reduces the inner diameter of the tracheosto-
my tube; thus, the imposed work of breathing for a spontaneously breathing is increased. Of note, if a fenestrated tracheostomy
tube is used, the inner cannula occludes the fenestraons unless there are also fenestraons on the inner cannula.
Fenestraon: The fenestrated tracheostomy tube is similar in construcon to standard tracheostomy tubes with the addion of an
opening in the posterior poron of the tube above the cu (Figure). With the inner cannula removed, the cu deated, and the nor-
mal airway passage inlet of the tube occluded (capped tube), the paent can inhale and exhale through the fenestraon and around
the tube, unless upper airway obstrucon precludes it. The cu must be completely deated before the tube is capped. In our experi-
ence, fenestrated tracheostomy tubes oen t poorly and thus do not always work as intended. The standard commercially available
tubes can signicantly increase ow resistance through the upper airway if the fenestraons are not properly posioned. Further-
more, the fenestraons may cause the formaon of granulaon ssue, resulng in airway compromise.
Subgloc sucon: Tracheostomy tubes that provide a sucon port above the cu are available. The subgloc suconing cannula is
located on the exterior surface of the cannula as a separate lumen, which can be connected to intermient or connuous sucon,
and is intended for the evacuaon of secreons situated above the tracheostomy tube cu (Figure, Table).
Conclusion:
The diversity of tracheostomy tubes reects the mulfaceted nature of paent needs in various clinical scenarios. Selecng the ap-
propriate type involves a careful consideraon of the paent's medical condion, neck and airway anatomy, ancipated duraon of
tracheostomy dependence, and the need for specic features such as cu inaon or fenestraon. Advances in tracheostomy tube
W A B I P N E W S L E T T E R
P A G E 7
technology are needed to take into account the unique requirements of each paent, ensure opmal outcomes, avoid complicaons
and enhances the overall quality of life of paents with indwelling tracheostomy tubes.
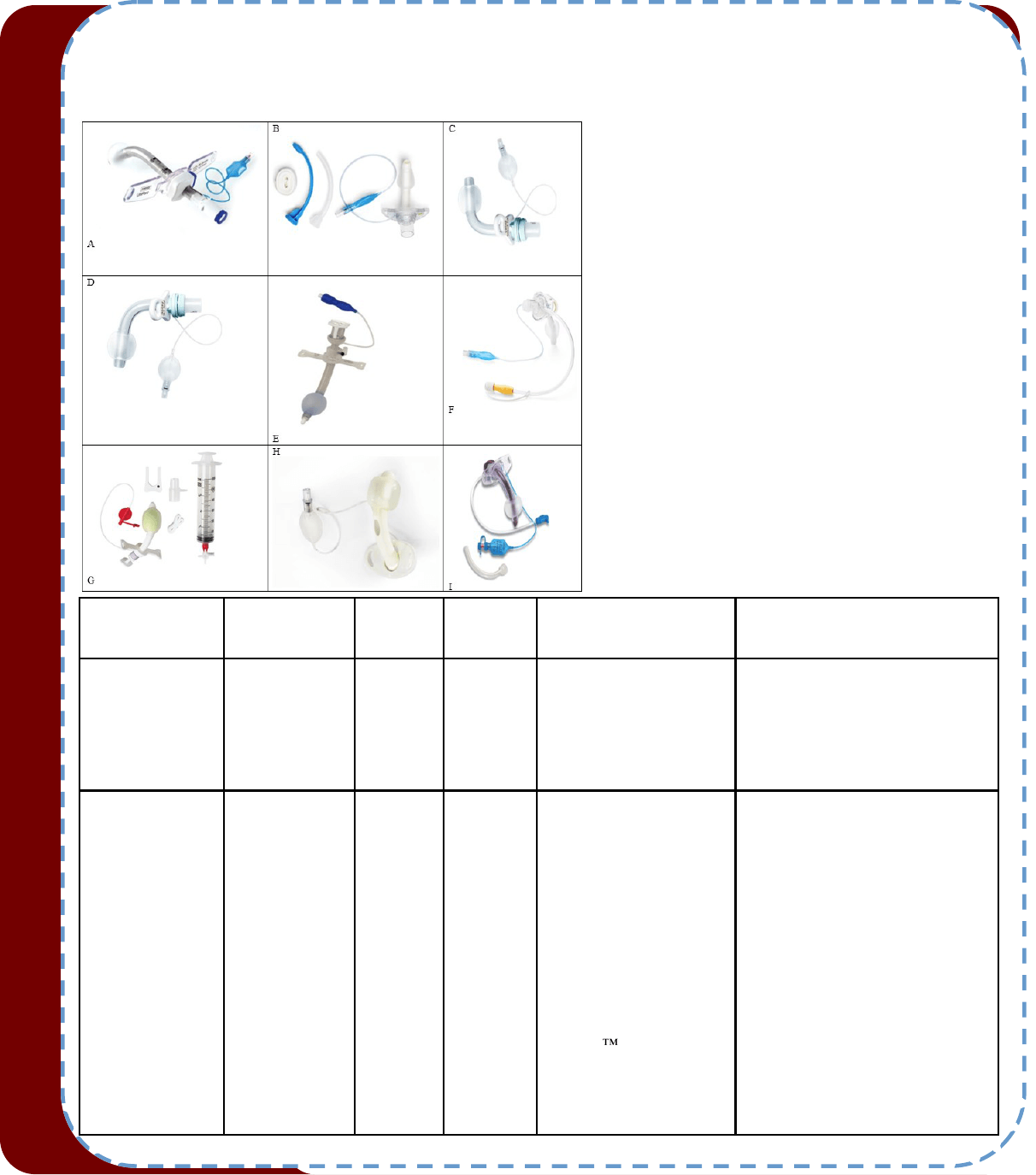
Figure 1. Types of cued tracheostomy tubes
A. Portex; B. Shiley; C Shiley Proximal XLT; D Shiley
Distal XLT; E. Bivona adjustable; F. Low Pressure, low
volume cu (Taper Guard); G. Foam cu; H. Fenes-
trated tracheostomy tube; I. Subgloc sucon port
tracheostomy tube
Tracheostomy
tube Name
Manufacturer Sizes
ID/OD
(mm)
Inner
Cannula
Cuff Comments
Bivona Tight-To-
Shaft (TTS) Tubes
Smiths Medical 6.0/8.8
7.0/10
7.5/10.5
8.0/11
8.5/11.8
9.0/12.3
Yes Low volume high pressure
Cuff
(LVHP), Tapered cuff
These cuffs are filled with
sterile water, not air.
“Tight-to-shaft” means when deflated,
the cuff lays flat against the shaft of
the trach tube. Recommended for pa-
tients being weaned from ventilation.
Bivona Aire-Cuff
Tubes*
Smiths Medical 6.0/8.8
7.0/10
8.0/11
9.0/12.3
9.5/13.3
Yes “Aire” indicates cuff to be
filled with air. These are
“mid-range” high-volume,
low-pressure cuffs (HVLP).
They come in tapered or
cylindrical shapes;
**Portex-Bivona regular
length, fixed and adjustable
tracheostomy tubes typically
available with TTS cuffs or
Aire-Cuf. Air-filled cuffs
designed to provide a secure
and comfortable seal. The
Aire-Cuf technology al-
lows for cuff inflation and
deflation to achieve an opti-
mal seal while minimizing
the pressure on the tracheal
wall
Recommended for patients on long
term ventilatory support. Inflatable
cuff is soft, flexible, and designed for
secure seal with minimal pressure on
the tracheal wall. Additional options
include talk attachment, fixed or ad-
justable flanges
W A B I P N E W S L E T T E R
P A G E 8
Bivona Fome-Cuf
Tubes
Smiths Medical 9.5/13.3 No Tapered cuff design.
A foam-filled cuff refers to
the presence of a cuff that is
filled with a soft, pliable
foam material. This cuff
places lower pressure on the
tracheal wall. It passively
inflates
Recommended for patients
with risk of tracheomalacia.
Cuff expansion adjusts to tra-
cheal wall changes while main-
taining a seal. Suitable for
long term use.
Caution: If the cuff breaks in
the patient, the the foam part of
the cuff cannot be deflated
Bivona Blu-Select
Tubes
Smiths Medical 6.0/9.2
7.0/10.5
7.5/11.3
8.0/11.9
8.5/12.6
Yes Tapered cuff, HVLP Tubes and packaging are color
coded by size
Bivona Portex Blue
Line Ultra Tubes
Smiths Medical 6.0/9.2
7.0/10.5
7.5/11.3
8.0/11.9
Yes HVLP cuff
Cylindrical shape
The Blue Line Ultra cuff is
designed to offer a secure seal
with minimal pressure, suitable
for long-term use
Bivona Portex Blue
Line Ultra Fenes-
trated
Smiths Medical 6.0/9.2
7.0/10.5
7.5/11.3
8.0/11.9
Yes HVLP, Cylindrical Needs a fenestrated inner can-
nula to function for speaking
purposes. Caution: Fenestra-
tions can become clogged up
with secretions.
Bivona Blue Line
Ultra Suction-aid
Tubes
Smiths Medical 6.0/9.2
7.0/10.5
7.5/11.3
8.0/11.9
Yes HVLP Cylindrical Incorporates a subglottic suc-
tion line
Bivona Uni-Perc
Adjustable Flange
Smiths Medical 8.0/12.6
9.0/13.6
Yes HVLP, Cylindrical
Recommended for patients
with long or thick necks. Al-
low tube length variation on
vertical and horizontal planes.
Shiley “Legacy”
Tracheostomy tube
Medtronic 5.0/9.4
6.4/10.8
7.6/12.2
8.9/13.2
Yes HVLP, Barrell-shape It uses Jackson sizing*
Shiley Flexible
tracheostomy with
taper-guard
Medtronic 6.5/9.4
7.0/10.1
7.5/10.8
8.0/11.4
8.5/12.2
9.0/12.7
10.0/13.8
Yes Taper-guard Low volume
Low Pressure (LVLP)
Integrated 15 mm adapter is
part of the trach, and this al-
lows the tracheostomy tube to
be connected to the ventilator
with or without inner cannula
in place
Shiley Proximal
Extended long tra-
cheostomy tubes
(XLT)
Medtronic 5.0/9.6
6.0/11
7.0/12.3
8.0/13.3
Yes HVLP Choose extra length in the
proximal portion to accommo-
date increased skin-to-tracheal-
wall distances in patients with
large neck circumference.
Shiley Distal XLT Medtronic 5.0/9.6
6.0/11
7.0/12.3
8.0/13.3
Yes HVLP Tubes with extended distal
length compensate for condi-
tions such as tracheal stenosis
or malacia, which often require
extra length to bypass the ab-
normal tracheal pathology
Shiley Fenestrated
tubes
Medtronic 5.0/9.4
6.4/10.8
7.6/12.2
8.9/13.8
Yes HVLP
Taper
Allows airflow through fenes-
tration for speech

W A B I P N E W S L E T T E R
P A G E 9
Table 1. Types of commonly used cued tracheostomy tubes and their features.
HVLP: High volume, low pressure
LVHP: Low volume, high pressure
LVLP: Low volume, low pressure
*There are two dierent methods for sizing tracheostomy tubes, and it's important to note that sizes among brands are not equivalent.
Jackson sizing is specic to Shiley regular and their exible tracheostomy tubes only. The size of the tracheostomy tube does not corre-
spond to any actual measurement of the tube. Internaonal sizing organizaon (ISO) is used by all other tracheostomy tube manufacturers,
including for Shiley XLTs. The size of the tracheostomy tube refers to the inner diameter of the tube without the inner cannula.
Note: Custom-made tracheostomies can be made based on bedside or radiologic measurements
References
1. Anand VK et al. Laryngoscope. 1992;102(3):237-243. doi:10.1288/00005537-199203000-00002
2. Sarper A et al. Texas Hear Inst J. 2005;32(2):154-158.
3. Grillo HC et al. J Thorac Cardiovasc Surg. 1995;109(3):486-493. doi:10.1016/S0022-5223(95)70279-2
4. Kapidzic A et al. Med Arh. 2004;58(6):384-385. doi:10.1016/s0022-5223(95)70279-2
5. Nseir S et al.. Eur J Anaesthesiol. 2009;26(3):229-234. doi:10.1097/EJA.0b013e3283222b6e
6. Maguire S et al. An in vitro comparison of tracheostomy tube cus Introducon: The Shiley
TM
Flexible adult tracheostomy tube with
TaperGuard
TM
cu has. Published online 2015:185-192.
Tips from the Experts
P A G E 10 V O L U M E 1 2 , I S S U E 1
Post Intubaon Tracheal Stenosis (PITS) is a well-described complicaon of endotracheal intubaon that can pose signicant challenges to
manage eecvely. Symptomac PITS can aect 1-5% of paents who are intubated and treatment should be tailored for each paent
based on a muldisciplinary approach considering non-surgical (endoscopic) and surgical intervenons (1, 2).
Herein we present a few strategies and technical ps from intervenonal pulmonology (IP) and thoracic surgery (TS) employed at the Uni-
versity of Chicago Medicine.
Indicaons
Paents may present with central airway obstrucve symptoms such as progressive dyspnea, wheezing/stridor, and diculty clearing secre-
ons. As a rule of thumb, nearly 50% narrowing of the cross-seconal area of the trachea is needed before an acve person experiences
dyspnea. Audible stridor usually occurs when the airway diameter is about 4-6 mm. Other causes of dyspnea should also be considered,
parcularly for paents previously on mechanical venlaon who may have sustained neuromuscular and/or pulmonary parenchymal con-
tribuons to their symptoms.
It is reasonable to aempt endoscopic management rst, parcularly for simple strictures (<1 cm in length and without associated malacia
(chondris)) without cricoid involvement. The success rate of laser-assisted mechanical dilaon in such cases is >60% (3). Surgical referral
should be pursued in paents who have cricoid involvement, have required mulple endoscopic intervenons, and in those with complex
lesions (>1cm, with malacia or full thickness injury) as recurrence is very high (80%) (1). Repeat endoscopic intervenons may lead to exces-
sive mechanical or thermal trauma that can worsen the extent of the stenoc segment and potenally convert operable paents to inopera-
ble (4). In such cases, paent- and lesion-specic factors should be evaluated to assess whether tracheal resecon is anatomically and physi-
ologically appropriate. In appropriately selected paents surgery has a high success rate >95% (1).
Paents should not undergo surgical resecon if they are “unt” for surgery due to poor cardiopulmonary reserve, dependent on mechani-
cal venlaon, have underlying chronic disease or anatomy which would lead to anastomoc failure or re-stenosis (e.g. on high dose ster-
oids, inammatory disease such as GPA, long-segment stenosis (longer than 4-5 cm)) (1). Poor surgical candidates will need a silicone stent
either long term (typically 12 months or longer) or unl they become operable (1). Up to a half of paents who undergo stenng may have
them removed without the need for addional intervenon, perhaps as a result of airway remodeling (1). Paents who cannot tolerate
stenng and are also not surgical candidates may be considered for tracheostomy.
Planning
Bronchoscopy is essenal for appropriate paent selecon and subsequent procedural planning. Specically, we use it to obtain precise
measurements and dene airway anatomy (length of stenosis, locaon in relaon to cricoid and carina). Bronchoscopy can also idenfy oth-
er eologies for stenosis (e.g. GPA, RP), the presence or absence of malacia, acve inammaon, and rule out laryngeal lesions (such as in-
adequate glos from stenosis, ulceraon, granuloma, vocal cord paralysis) which would limit the success of tracheal intervenons.
Our typical pracce is to perform airway assessments with a exible bronchoscope. The seng and need for an arcial airway depend on
Management of Post Intubaon Tracheal Stenosis:
ps from a mul-disciplinary airway team
Sepmiu Murgu
Department of Medicine,
Division of Pulmonary and
Crical Care
The University of Chicago
Gaurav Ajmani
Department of Medicine,
Division of Pulmonary and
Crical Care
The University of Chicago
Maria Lucia Madariaga
Department of Surgery,
Division of Cardiothoracic Surgery
The University of Chicago
Tips from the Experts
P A G E 11 V O L U M E 1 2 , I S S U E 1
the operator’s preference and clinical scenario. We prefer to perform this under moderate sedaon so the paent can cooperate with vari-
ous respiratory maneuvers (deep inhalaon, forced exhalaon, coughing) which allow detecon of concurrent airway malacia or funconal
obstrucon. In an anesthezed paent we aempt to simulate this by applying sucon. Paents who are in respiratory distress are typically
taken directly to the OR as below (see Urgent Management). Addional workup includes serologic tesng for GPA, CT neck/chest to evaluate
for evidence of other airway pathology, and pulmonary funcon tesng with evaluaon of ow-volume loops and assessment of sing/
supine symptoms and forced vital capacity.
In all paents, management of concurrent or exacerbang condions should also ideally be opmized, including acid reux, cardiac disease
or volume overload, and obstrucve lung disease prior to invasive intervenons directed at PITS. Prior to surgical intervenon, chronic ster-
oids should be weaned, and diabetes mellitus should be controlled.
Procedure
Endoscopic treatment typically involves a combinaon of thermal therapy to cut the scar/stricture followed by gentle dilaon. Thermal thera-
pies include KTP laser or electrocautery knife or needle and in our pracce both are employed based on equipment availability and ability to
appropriately align the tool with the lesion in the airway. We will typically make anywhere from 1-3 radial incisions into an area of scar or
stricture depending on the extent of involvement. Dilaon following thermal therapy is likely to be more eecve than dilaon alone in
opening the airway and delaying recurrence. In addion, dilaon without prior radial incision will result in excessive mechanical trauma
which by itself can promote recurrence. Dilaon may be performed with commercially available dilang balloons and/or a rigid bronchoscope
if one is employed [Figure 1]. Occasionally, we use endotracheal tubes of increasing size or Jackson dilators, especially if working in conjunc-
on with ENT and the paent is under suspension laryngoscopy (for high stenoc lesions). In paents who had a signicant benet but expe-
rience a recurrence, we will proceed with a maximum of 3 repeat endoscopic intervenons while they undergo evaluaon for surgical candi-
dacy. We will also consider intra-lesional steroid injecon under direct visualizaon (40mg of triamcinolone) in paents who recur with evi-
dence of inammaon at me of repeat bronchoscopy.
Silicone stents improve respiratory symptoms, however migraon and mucus occlusion are important adverse consideraons. Further, plac-
ing an appropriately sized silicone tracheal stent requires an adequately sized rigid bronchoscope, which in our experience is not always easy
to insert and maneuver. A smaller rigid tube may only permit placement of a smaller diameter stent that is more prone to migraon. Mucus
plugging can also be an issue if paents are not adherent with saline nebulizers. We therefore typically reserve the use of silicone stents long-
term for paents whose disease is not amenable to thermal therapy/dilaon and who are not surgical candidates. Bare metal stents carry a
black box warning by the U.S. Food and Drug Administraon for benign airway stenosis and should not be used.
Surgical management involves either laryngotracheal resecon (if the cricoid is involved) or tracheal resecon, followed by reconstrucon. In
our instuon, we use cross-eld venlaon and total intravenous anesthesia. Aer adequate exposure of the trachea through a collar inci-
sion, the stenoc segment is resected. Stay sutures are placed so that intermiently the surgeon can check the level of anastomoc tension
by approximang the 2 cut ends of trachea. Once sased with resecon, the anastomosis is performed using absorbable suture. Muscle
buress aps are placed to protect the anastomosis and a chin stch (“Grillo stch”) is applied to remind the paent not to extend the neck
excessively. Surveillance bronchoscopy is performed on postoperave day 7 to assess the integrity of the anastomosis [Fgure 2].
Urgent management
Symptomac paents with a crical airway may require urgent intervenon without the extensive prior evaluaon detailed above. We favor
transferring these paents to the ICU and temporizing with upright posioning and consideraon of posive airway pressure and/or heliox
(eecve at 80:20 or 70:30 mix and should not be used if the paent requires more than 30% oxygen ). Intubaon or bronchoscopy at the
bedside should be avoided when paents are crical, especially if there is a lack of advanced equipment and personnel availability. Securing
the crical airway should be done in the operang room with readiness to use a rigid bronchoscope if needed. Surgical teams may be needed
on standby to access the airway if this is not possible from above depending on operator experience and instuonal process. In appropriate
paents who are markedly and rapidly decompensated, extracorporeal support (ECMO) may also be considered, though in our experience
this has not been necessary with a muldisciplinary airway team. There is no role for emergent tracheal resecon and reconstrucon.
Quality Control
We conduct thorough pre-procedural assessments as above aimed at conrming that a paent’s symptoms are most likely from PITS, that
contribung and comorbid factors are well managed. Muldisciplinary meengs are the norm in our instuon and oen paents undergo
Tips from the Experts
P A G E 12 V O L U M E 1 2 , I S S U E 1
joint procedures by two or more airway specialists (IP, ENT and TS). These discussions as well as pre-intervenon bronchoscopy aid greatly in
personalizing treatment and assuring avoidance of unnecessary repeated endoscopic procedures for complex lesions or premature surgical
resecon of simple strictures that would have otherwise responded to laser-assisted mechanical dilaons. With all intervenons, we will typi-
cally perform surveillance exible bronchoscopy – around 1-3 months following endoscopic intervenon, and for surgical paents at 1 week
and 3 months post-op.
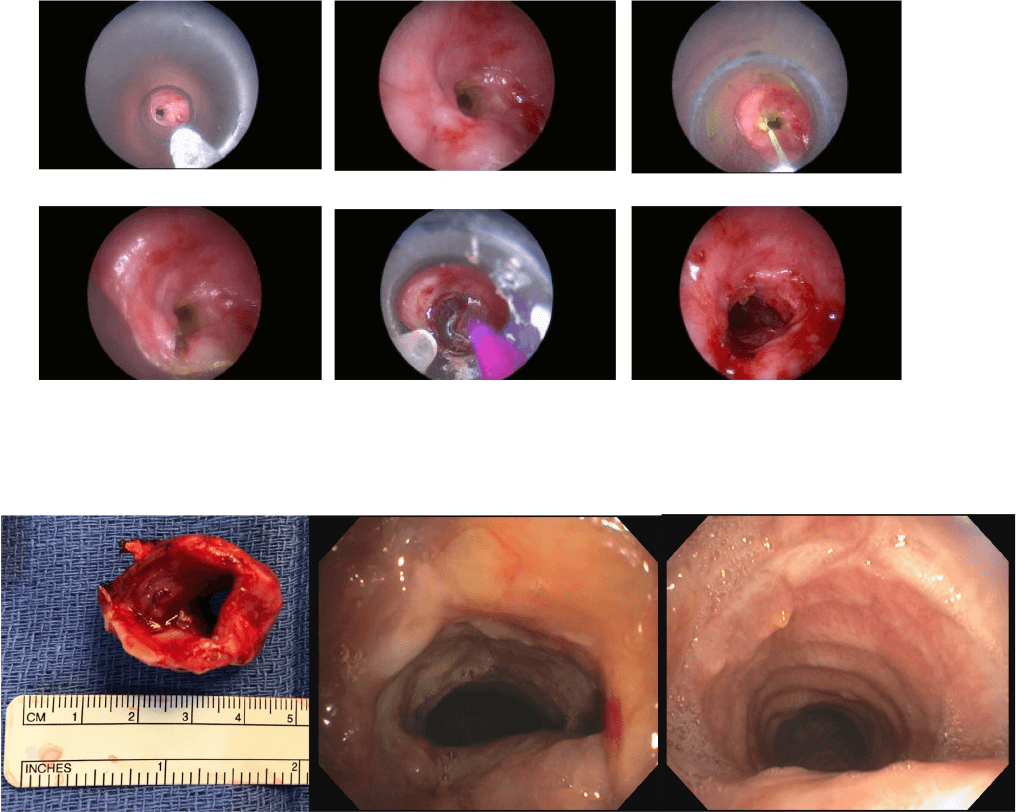
Figure Legend
Figure 1. Complex, circumferenal tracheal stenosis seen during rigid bronchoscopic intubaon (top le) and close view (top center). This was managed by
laser assisted mechanical dilaon. The stricture was cut using KTP laser for two radial incisions (top right and boom le images). In this case, we decided to
inially use a balloon for the dilaon ( boom center) as the stricture felt very hard, and we try to avoid both mechanical and thermal trauma when manag-
ing these paents. The airway patency was restored (boom le).
Figure 2. Resected tracheal stenosis segment showing “full thickness” airway involvement, unlikely to resolve with mulple dilaons (le). Bronchoscopy at
day 7 (center) and 3 months post op (right) showing healed anastomosis and no recurrence.
References
1. Agrawal A et al. Respir Med. 2021;187:106582.
2. Murgu SD et al. Endobronchial Prostheses. In: Díaz-Jimenez JP, Rodriguez AN, editors. Intervenons in Pulmonary Medicine. Cham: Springer Interna-
onal Publishing; 2018. p. 213-41.
3. Mehta AC et al. Chest. 1993;104(3):673-7.
4. Gaissert HA et al J Thorac Cardiovasc Surg. 2003;126(3):744-7.
5. Grillo H.C. (2003). Posntubaon Stenosis. In H.C. Grillo (Eds.), Surgery of the Trachea and Bronchi. (1
st
ed., pp. 301-339). B.C. Decker.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 13
Internaonal Humanitarian Law and the Israel-Palesne Conict
Most of people are likely to nd it challenging to maintain raonality amidst the overwhelming sense of sorrow that accom-
panies the recent events in Israel and Gaza.
Even if the Hamas incursion and Israel's siege and shelling of the densely populated Gaza Strip connue to cause crimes and
deaths, internaonal law can guide an examinaon of the current situaon. New informaon is released daily. Verifying spe-
cics takes me, disinformaon is widespread, and debates about unsubstanated claims may get boring. War rules deter-
mine what maers and what should happen next.
In fact, the exceedingly complex situaon in the Gaza Strip has led to discussions over whether both groups' acvies vio-
late internaonal humanitarian law. Like many other subjects, the public, communicators, and media voice strong opinions
without knowing internaonal humanitarian law or how it applies to this conict's protagonists. Emoons, prejudices, geo-
polical interests, and polical posionings drive polical leaders, human rights advocates, and ordinary individuals to view
informaon dierently. Dierent judicial bodies may rule dierently on the same text, as with any legal theory. This form of
inescapable ambiguity is not exhausve, as many civil, criminal, and internaonal legal situaons are clearly right or wrong.
Internaonal humanitarian law comprises a set of regulaons aimed at migang the impact of armed conicts for humani-
tarian reasons. It safeguards individuals who are not acvely parcipang in hoslies and imposes limitaons on the meth-
ods and means of warfare. Addionally known as the law of war or the law of armed conict, internaonal humanitarian law
is an integral component of internaonal law, which governs the interacons between sovereign states. This body of law is
delineated in agreements such as treaes or convenons, customary rules derived from state pracces seen as legally bind-
ing, and general principles.
The scope of internaonal humanitarian law is restricted to armed conicts and does not dictate whether a state is per-
mied to employ force; this aspect is governed by a disnct secon of internaonal law outlined in the United Naons Char-
ter. While the roots of humanitarian law trace back thousands of years, the modern version, encapsulated in the Geneva
Convenons of 1949 and other treaes, has evolved over me. The universal codicaon of these laws commenced in the
nineteenth century, with states progressively agreeing upon praccal rules shaped by the harsh lessons of contemporary
warfare. These rules aim to strike a delicate balance between humanitarian consideraons and the military needs of states.
Today, internaonal humanitarian law represents a universally recognized body of legal principles.
Nearly every government has signed the Fourth Geneva Convenons of 1949 and the 1977 Addional Protocols that protect
vicms in armed conicts and enhance these Convenons.
Various agreements restrict certain weapons and military methods while protecng parcular organisaons and assets as
the 1954 Convenon for the Protecon of Cultural Property in the Event of Armed Conict, the 1972 Biological Weapons
Convenon, the 1980 Convenonal Weapons Convenon with its ve protocols, the 1993 Chemical Weapons Convenon,
the 1997 Oawa Convenon on an-personnel mines, and the 2000 Oponal Protocol to the Convenon on the Rights of
the Child on child involvement in armed
Many parts of internaonal humanitarian law are customary law, binding on all governments. This legislaon only applies to
military conicts, not internal tensions or isolated violence. Aer a disagreement begins, the law applies imparally to all
sides. Internaonal humanitarian law disnguishes between internaonal (IAC) and non-internaonal armed conicts
(NIAC), with the former involving at least two naons and operang under the Fourth Geneva Convenons and Addional
Protocol I. On the other hand, non-internaonal armed conicts refer to hoslies that are limited to the territory of a single
State and include either convenonal armed forces combang armed dissident organisaons or armed groups engaging in
combat with each other.
There is oen a misconcepon regarding the interchangeability of humanitarian law with human rights law. It is essenal to
dierenate between them. While there may be some parallels in their legislaon, these two legal systems have developed
separately and are covered by separate treaes. Human rights legislaon is specically valid during periods of peace, in con-
trast to internaonal humanitarian law. However, some provisions under human rights law may be temporarily suspended
during mes of armed conict.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 14
The rules of law are non-reciprocal, meaning they are applicable regardless of the acons of the opposing party. Violaons,
such as intenonally targeng civilians or imposing collecve punishment, cannot be jused by arguing that another party
has commied violaons or that there are power imbalances or other injusces.
The primary principle of internaonal humanitarian law during armed conicts is that all pares are obligated to consistently
dierenate between combatants and civilians. It is imperave to refrain from targeng civilians and civilian enes. Pares
involved are only allowed to target combatants and military objecves. It goes as far as considering that merely asserng
that civilians are not the intended vicms of the aack is insucient. According to internaonal humanitarian law, the par-
es involved in the conict are obligated to take all praccal measures to reduce injury to people and civilian infrastructure.
Aacks that do not disnguish between combatants and civilians or that are likely to cause excessive harm to civilians rela-
ve to the military advantage are strictly forbidden.
Prisoners of war and maimed, stranded, or unwell combatants who have ceased parcipaon are also safeguarded under
internaonal humanitarian law. Respect for the physical and mental health of individuals belonging to these parcular
groups is warranted, on account of their mere existence. Ensuring the protecon and compassionate treatment of individu-
als without any form of discriminatory treatment is of the utmost importance.
It is strictly prohibited to intenonally inict death or injury upon an adversary who surrenders or becomes incapacitated
during combat. The party in a posion of authority is responsible for gathering and providing medical assistance to individu-
als who are injured or unwell. Under no circumstances are aacks on medical personnel, medical supplies, hospitals, or
healthcare instuons permied.
The IHL species that it is imperave to ensure the safeguarding of all ambulances. Addionally, there exist comprehensive
regulaons that dictate the specic requirements for the connement of prisoners of war and the treatment of civilians. This
include the supply of sustenance, lodging, and healthcare, as well as the entlement to communicate with their relaves.
The legislaon establishes a variety of unambiguous symbols that can be employed to disnguish individuals, locaons, and
items that are under protecon. The primary symbols include the red cross, the red crescent, and the emblems that desig-
nate cultural property and civil defence instuons.
Furthermore, internaonal humanitarian law strictly forbids any taccs or strategies used in bale that do not disnguish
between combatants and non-combatants, such as civilians. It is also crucial to prevent any excessive harm or avoidable
suering. Humanitarian law has therefore banned the use of many weapons, including exploding bullets, chemical and bio-
logical weapons, blinding laser weapons and an-personnel mines.
The laws of war require pares engaged in combat with the intent to damage civilians to furnish "eecve advance warn-
ing," unless the situaon renders such acon unfeasible. However, issuing a warning does not absolve any party of the re-
sponsibility to protect civilians. Civilians who do not evacuate remain protected despite having been issued a warning. Main-
taining their anonymity is of the utmost importance, and assailants must implement every feasible measure to protect them.
Statements that are not genuine warnings and instead seek to induce dread in the public through the use of threats of vio-
lence in order to coerce them into evacuang are strictly prohibited.
The signicance of Internaonal Humanitarian Law transcends naonal boundaries and precludes any exempon for mili-
tary, security, or naonal consideraons. This is because military imperaves are already duly considered in all instruments
of internaonal humanitarian law, which reconcile military necessity with human demands. The Internaonal Commiee of
Red Cross (ICRC) Commentary on the 4th Geneva Convenon states that: "… no Contracng Party can oer any valid pretext,
legal or otherwise, for not respecng the Convenon in its enrety. ('In all circumstances') also means that the applicaon of
the Convenon does not depend on the nature of the conict. "In addion, Arcle 27 of the Vienna Convenon points out
that "a party may not invoke the provisions of its internal law as juscaon for its failure to perform a treaty."
Despite the existence of notable cases in which internaonal humanitarian law has successfully protected civilians, prison-
ers, the injured, and the inrm, as well as restricted the use of cruel weapons, it is evident to an unbiased observer that
breaches of internaonal humanitarian law are numerous and on the rise. Civilians are increasingly becoming the principal
casuales of warfare and are enduring incalculable suering.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 15
Evidently, substanal obstacles will inevitably be encountered in the enforcement of this legislaon, given that it is designed
to be implemented during periods of profound unrest. However, it is equally apparent that the internaonal community
employs dierenal standards in its eorts to ensure eecve compliance with regulaons based on geopolical or alliance
consideraons.
The issue of the Israeli-Palesnian conict is notably sensive. Palesne's complex history of conicng claims, numerous
geopolical interests in the Middle East, ambiguous legal status of Palesnian territories, divergent posions within the in-
ternaonal community, the unconvenonal armed force status of Hamas (considered a terrorist organisaon by many
states), and misinterpretaons of opinions regarding Israel's foreign policy as those regarding the Jewish people all contrib-
ute to this complexity. Therefore, in addion to the inherent technical challenges associated with interpreng the implemen-
taon of Internaonal Humanitarian Law (IHL) in this intricate situaon, the conduct of each party operang within that legal
structure is subject to varying interpretaons among scholars, policymakers, polical gures, and ordinary cizens world-
wide.
The unique Israeli-Palesnian conict, agreements, and memoranda have created a lex specialis regime that governs all as-
pects of their relaonship, including the status of each party in relaon to the territory. The UN Resoluon adopted by the
General Assembly on 9 December 2015 (on the report of the Special Polical and Decolonizaon Commiee) declared that
UN: 1) Rearms that the Geneva Convenon relave to the Protecon of Civilian Persons in Time of War, of 12 August
1949, is applicable to the Occupied Palesnian Territory, including East Jerusalem, and other Arab territories occupied by
Israel since 1967 and 2) Demands that Israel accept the de jure applicability of the Convenon in the Occupied Palesnian
Territory, including East Jerusalem, and other Arab territories occupied by Israel since 1967, and that it comply scrupulously
with the provisions of the Convenon;
In spite of that, in the opinion of Peter Maurer, President of the Internaonal Commiee of the Red Cross in 2012 (so be-
fore the Hamas aack and declaraon of war by Israel), the recurrent claim that the Fourth Geneva Convenon applies to
the territories ignores the unique posion of Palesne and this essenal body of accords and as Israeli-Palesnian agree-
ments require a nal status negoaon to determine territory fate, so he called the ICRC and the internaonal community to
remain neutral and not prejudge the conclusion.
Assisng Professor Jérôme de Hempnne of Utrecht University conducts an exhausve analysis of whether the NIAC or IAC
branch of Internaonal Humanitarian Law pertains to the hoslies between the Israeli and Hamas military wing in Gaza.
Under IHL, the classicaon of these conicts is conngent on whether Palesne is a state and Gaza is an occupied territory.
According to him, this categorizaon is vital for establishing the legal framework that safeguards the rights and obligaons of
individuals and combatants. The applicability of the IAC and NIAC's hoslies laws at this juncture of the conict is now com-
parable as a result of customary IHL. Regarding the accountability of violators of internaonal humanitarian law (IHL) under
internaonal criminal law, they diverge. His analysis concludes that the enre Gaza conict ought to be governed by the one
-of-a-kind IAC system. This method also strengthens legal protecon for hoslies-threatened persons and property. The
Internaonal Criminal Court (ICC) would then be competent to prosecute and try several important war crimes that fall un-
der its jurisdicon only if they are commied in IAC, such as disproporonate aacks, using human shields, or using starva-
on as a weapon. The enre regime of protecon in 4
th
Geneva Convenon would benet civilian populaons on both sides,
and the ICRC would have regular access to all detainees to verify their condions and restore family links without belligerent
consent (Rule 124 of ICRC Customary Law Study).
Since October 7, Hamas and its supporters have launched hundreds of missiles from Gaza onto Israel, and have breached the
Gaza-Israel border barrier on October 7, capturing Israeli military checkpoints and invading Israeli communies and Kibbutz-
es. They massacred hundreds and abducted 220 troops and civilians to Gaza. Aer Israeli bombings on Gaza began, Hamas
vowed to kill a capve if Israel targeted houses without noce. These violent acts likely constuted IHL breaches under Art. 7
of the Rome Statute of the Internaonal Criminal Court (intenonal killings, unlawful imprisonments, and civilian hostage-
takings may be war crimes under Rome Statute). Aer Palesne joined the Rome Statute in April 2015, the Internaonal
Criminal Court has jurisdicon over war crimes perpetrated on Palesnian territory and by Palesnians, including Hamas and
PIJ members. Addionally, Art. 34 of the Fourth Geneva Convenon and Art. 3 of the Four Geneva Convenons ban the kid-
napping of hostages in internaonal and non-internaonal conicts.
On the other hand, the day aer Hamas-led strikes, Israeli Prime Minister Benjamin Netanyahu declared war and retaliated.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 16
He stated Israel wanted to annihilate Hamas's Gaza military. Israeli Defence Minister Yoav Gallant then said that he will block
o Gaza since airpower would not be adequate to bale Hamas. Instead, Gaza Strip supplies must be cut o. No food, ener-
gy, gasoline, medicaon, or drinking water has been transported to Gaza over Israel's border since October 9, 2023. Prime
Minister Netanyahu has stated that Israel will not provide help unl Hamas releases the hostages. On October 12, 2023, the
Gaza Strip's lone electrical plant stopped down due to fuel shortages. This caused the public electrical supply to collapse,
aecng health and drinking water.
Prime Minister Netanyahu urged Gazan civilians to ee bale zones before the air aacks. On October 13, the Israeli military
ordered civilians and foreign organisaons to evacuate the northern Gaza Strip within 24 hours in preparaon for an intensi-
ed air campaign or land invasion. In contrast, the Hamas-led administraon urged residents to stay in northern Gaza, ac-
cording to the Israeli military. The UN and human rights organisaons asked for the Israeli statement to be withdrawn since
a mass evacuaon of 1.1 million people was unachievable in 24 hours.
Aer those events, Gaza's civilian populaon has few safety opons. The UN has no civilian shelters or bunkers, although a
few hundred thousand have found refuge in hospitals. Only lile supplies and protecon are guaranteed there. Rafah, the
Palesnian border crossing to Egypt, is restricted to Gazans who wish to ee and has been bombarded by Israel mulple
mes. Hamas has released few hostages into Egypt.
Regardless maer who started the war, internaonal humanitarian law applies to all sides. What internaonal law allows in
an armed confrontaon does not rely on whether the side is an aggressor or defence. The only purpose is to safeguard civil-
ians, medical sta, journalists, and cultural property. Indiscriminate assaults (those that target civilians and ghters) must be
prevented to guarantee this protecon. This restricon applies to all armed conicts and is codied in Art. 48 of the First and
Second Addional Protocols to the Geneva Convenons. Hospitals and medical sta are protected from military strikes if
designated properly. Violaon of this ban is a war crime under Rome Statute Art. 8.
Due to connuous ghng with Israel and Egypt closing border crossings, Gaza Strip civilians cannot exit the blockade. Egypt
permied some Palesnians to ee Gaza in the early days of the military assault but has subsequently closed the border.
Siege warfare—starvaon of enemy civilians—is also illegal in all armed conicts. This implies that only a valid military goal
may be locked down or sieged. Civilians may not be targeted by the siege, and basic items may be supplied. Even if combat-
ants could get food, it shouldn't be blocked. A complete shutdown, which makes it impossible to supply Gaza’s civilian popu-
laon with food, drinking water and medicines, is, unlike prevenng the import of fuel or the supply of electricity, under no
circumstances proporonate and permissible under internaonal law. Not least, the blockade of supplies vital for life is a
collecve punishment
in accordance with Art. 33 of the Fourth Geneva Convenon and hence violates internaonal humani-
tarian law.
The commitment to Israel's security, condemnaon of Hamas's atrocies, and support for Israel's goal of eliminang Hamas
do not exempt it from internaonal law. Thus, the internaonal community should use its close relaons to Israel to nego-
ate hostage release. It should also establish protecon zones, refrain from using prohibited warfare methods, ensure hu-
manitarian access (and halt violence for humanitarian purposes), and facilitate the delivery of drinking water, food, medi-
cines, and hospital generator fuel to all of Gaza. For medical emergencies and internaonal civilian evacuaon, humanitarian
corridors are needed. Simultaneously, states with es to Hamas, such as Egypt and Qatar, must pressure the group to pro-
tect hostages, advocate for their release, stop rocket re at Israel, and allow civilians to evacuate combat zones.
We should all be outraged by Hamas' October 7th strikes on Israel. Jusce, responsibility, and retribuon for these horrible
killings, the safe repatriaon of capves, and a halt to strikes into Israel must be demanded. However, channelling anger and
anguish towards innocent people, like the 99 United Naons Relief and Works Agency for Palesne Refuges (UNRWA) sta
members who died, cannot preserve peace and security. Some events taking place in the Gaza strip are obscene, and heart-
breaking.
The Israeli government has garnered support from the majority of Western naons since the commencement of the conict.
But over me, several events that many interpret that violate Internaonal Humanitarian Law (IHL) and are deemed taboo
have caused signicant concern, cricism, and calls for acon to stop the bloodshed. Israel's military oensive in Gaza, char-
acterised by the use of powerful explosive weapons that have destroyed tens of thousands of structures, is having signicant
humanitarian and human rights repercussions, as acknowledged by various polical leaders, scholars, and UN agency sta,
despite ongoing polical backing.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 17
A considerable number of experienced humanitarian workers who are currently on the eld nd it dicult to fully grasp the
abhorrent condions to which they and the local populace are being exposed. The casuales incurred by humanitarian work-
ers during this conict, in the rst four weeks, surpassed the cumulave toll of humanitarian workers throughout the Syrian
civil war that has aicted the region for the past four years. Intenonally singled out hospitals include Al Shifa Hospital and
the Indonesia Hospital; the severity of these assaults on medical facilies is truly disconcerng. The road infrastructure in the
vicinity has been signicantly impaired due to the strikes, thereby impeding access to the facility. Addional evacuaon di-
recves have been promulgated for certain establishments, in conjuncon with the overarching instrucons for all inhabit-
ants of northern Gaza to evacuate. Nevertheless, these evacuaons, which contravene World Health Organisaon recom-
mendaons, are tantamount to a "fatal sentence" in southern Gaza, where hospitals are unable to accept addional paents
due to the total collapse of the healthcare infrastructure.
Under internaonal humanitarian law, medical units must always be protected and respected, with access to humanitarian
assistance in its many forms—food, water, and medical supplies—guaranteed in parcular. Any Palesnian armed group that
defends itself with civilians or property is in violaon of war laws. The conduct exhibited by Palesnian armed groups does
not absolve Israel (or any other country in similar circumstances) of its responsibility to safeguard civilians and maintain dis-
ncon, proporonality, and safeguards in the face of assault. Neglecng to do so constutes a breach of military regula-
ons. A considerable number of targeted individuals are in no way associated with violaons commied by armed groups
aliated with the state or non-state. Reducing or eliminang civilian rights in response to the acons of armed groups over
which they have no authority would be illogical.
Self-defense, as invoked by Israel in its response, stands as one of the juscaons for war, with Arcle 51 of the UN Charter
safeguarding this right "if an armed aack occurs". The exercise of this right of self-defense, nevertheless, connues to be
governed by internaonal humanitarian law. State enes are obligated by jus in bello (jusce in war) to alleviate suering
during armed conicts; the lawful exercise of self-defense does not authorise unrestricted use of force. The humanitarian
agencies' asseron that both sides should adhere to the principles of Internaonal Humanitarian Law (IHL) does not imply a
crical assessment of the Israeli government's decision to conduct a military operaon, a lessening of the internaonal com-
munity's outrage over the inial Hamas aack, or an endorsement of one side or the other in the conict. Jus in bello
(internaonal humanitarian law), is merely the body of legislaon that governs the course of hoslies. Its solely humanitari-
an objecve is to alleviate the suering that armed conicts inict. It operates autonomously from the movaons or raon-
ales that drive war, as dictated by jus ad bellum. Furthermore, it is not the intenon of humanitarian actors to comment on
polical and legal issues aecng the status of Territories and who is entled to what. However, defending the lives and dig-
nity of aid workers and noncombatants is a crical component of our mission, and we would be failing miserably to our du-
ty if we did not remind both sides of their respecve use-of-force restricons and demand both sides to honour their com-
mitments.
Those who have extensively engaged with press or social media recently may have observed individuals intertwining the
righteousness of the conict itself with the righteousness of its conduct. Some seem to jusfy the killing of Israeli civilians by
condemning Israel's occupaon of Palesnian territories, while others seem to downplay the killing of Palesnian civilians in
airstrikes, asserng Israel's right to self-defense.
Approaching causes and conduct as disnct maers, as the law does, serves as a method to maintain a clear focus on the
intricacies of war and the underlying polical quesons, without losing sight of the shared humanity on all sides. In the
words of Josep Borrell, the head of foreign policy for the European Union, "Israel has the right to defend itself, but it must do
so in compliance with internaonal and humanitarian law."
Furthermore, this duty of protecon safeguards humanity against its darkest demons, as well as against the disgrace and
degradaon of the human race, in addion to ensuring the lives and welfare of the aected populace. Beyond the scope of
any legislaon, violence, bodily injury, fear, hunger, and harm perpetrated on defenceless persons incapable of reprisal are
not acceptable under the universal moral code. While this does not imply that it has never occurred before, it does indicate
a setback in the development of a moral community. Regardless of the severity of an individual's crimes, even in mes of
peace and across vastly diverse cultures, the criminal jusce system emphasises the value of every human life,. Disrespect
for human life inicts severe suering upon the vicms, but inicts an even greater harm upon the human condion and
community membership of those who commit such acons, which are illegal but primarily immoral in nature.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 18
The Gazan people are currently completely dependant on internaonal aid; but, with no gasoline, electricity, food, or water,
and a besieged region, humanitarian assistance is impossible to deliver. Almost all humanitarian assistance currently de-
pends on UNRWA, whose capacity is nearing the brink of collapse. Characterising the daily situaon in Gaza as inhumane
would be an inaccurate and insucient portrayal. A universal senment among humanitarian workers who have recent-
ly worked in Gaza—and all of them with extensive experience and, unfortunately, a sombre history of witnessing atrocies—
is "I never imagined something of this magnitude was even possible."
As a result, an increasing number of non-governmental organisaons, United Naons ocers, humanitarian aairs experts,
and scholars of internaonal humanitarian law are speaking out in support of an immediate ceasere and suspension of the
siege so that adequate aid can be delivered. We do not inquire about the resoluon of the conict or oer suggesons on
how it ought to be carried out. We refrain from discussing or expressing public views regarding the legal ramicaons of the
manner in which the war was conducted. We simply implore the cessaon of violence, the guarantee of protecon for hu-
manitarian personnel, and the provision of secure access for all recipients of humanitarian aid. We peon for the provision
of shelter, food, water, medical care, and medical aenon, the release of the capves, and the prevenon of any human
rights violaons that may be brought before the courts.
In addion to the exceedingly perilous repercussions that may befall thousands upon thousands of individuals not only in the
region but also in neighbouring or remote naons, we are currently observing one of the most abhorrent humanitarian ca-
tastrophes during a modern war. Indeed, we are not merely losing human lives; we are also profoundly losing the scant rem-
nants of humanity that remain on this planet.
We cannot aord to remain indierent. We do not advocate for an idealised or romancised future; rather, we cauon that
failure to establish a minimally more peaceful and compliant global order will render all regions unsafe, because no locaon
is immune to violence in an inhumane world where we forget that even war has rules.
References
1. Convenon (IV) relave to the Protecon of Civilian Persons in Time of War. Geneva, 12 August 1949.hps://ihl-databases.icrc.org/
en/ihl-treaes/gciv-1949 (accessed December 12, 2023)
2. Protocol Addional to the Geneva Convenons of 12 August 1949, and relang to the Protecon of Vicms of Internaonal Armed
Conicts (Protocol I), 8 June 1977. hps://ihl-databases.icrc.org/en/ihl-treaes/api-1977 (accessed December 12, 2023)
3. Arnold R et al.. Internaonal Humanitarian Law and Human Rights Law: Towards a New Merger in Internaonal Law. 2008
4. Carey J et al. Pritchard R (ed). Internaonal Humanitarian Law: Prospects. Transnaonal Publishers Inc. New York, 2006
5. Ba Aker – Internaonal humanitarian law, ICRC and Israel’s status in the Territories Internaonal Review of the Red Cross.
doi:10.1017/S181638311300060X
6. Hempnne Jérôme Classifying the Gaza Conict Under Internaonal Humanitarian Law, a Complicated Maer. European Journal of
Internaonal Law (Oxford). November 2023, hps://www.ejiltalk.org/classifying-the-gaza-conict-under-internaonal-humanitarian-
law-a-complicated-maer/ (accessed December 13, 2023)
7. Asseburg, Muriel; Wiese, Lisa: Hamas’ Atrocies, Israel’s Response, and the Primacy of Internaonal Law to Protect Civilians,
VerfBlog, 2023/10/31, hps://verfassungsblog.de/protect-civilians/, DOI: 10.59704/597372b78adb07fc.
*The views expressed in this arcle are those of the author (Silvia Quadrelli) and do not necessarily reect the ocial posi-
ons of the Execuve Board or Internaonal Board of Regents of the WABIP.
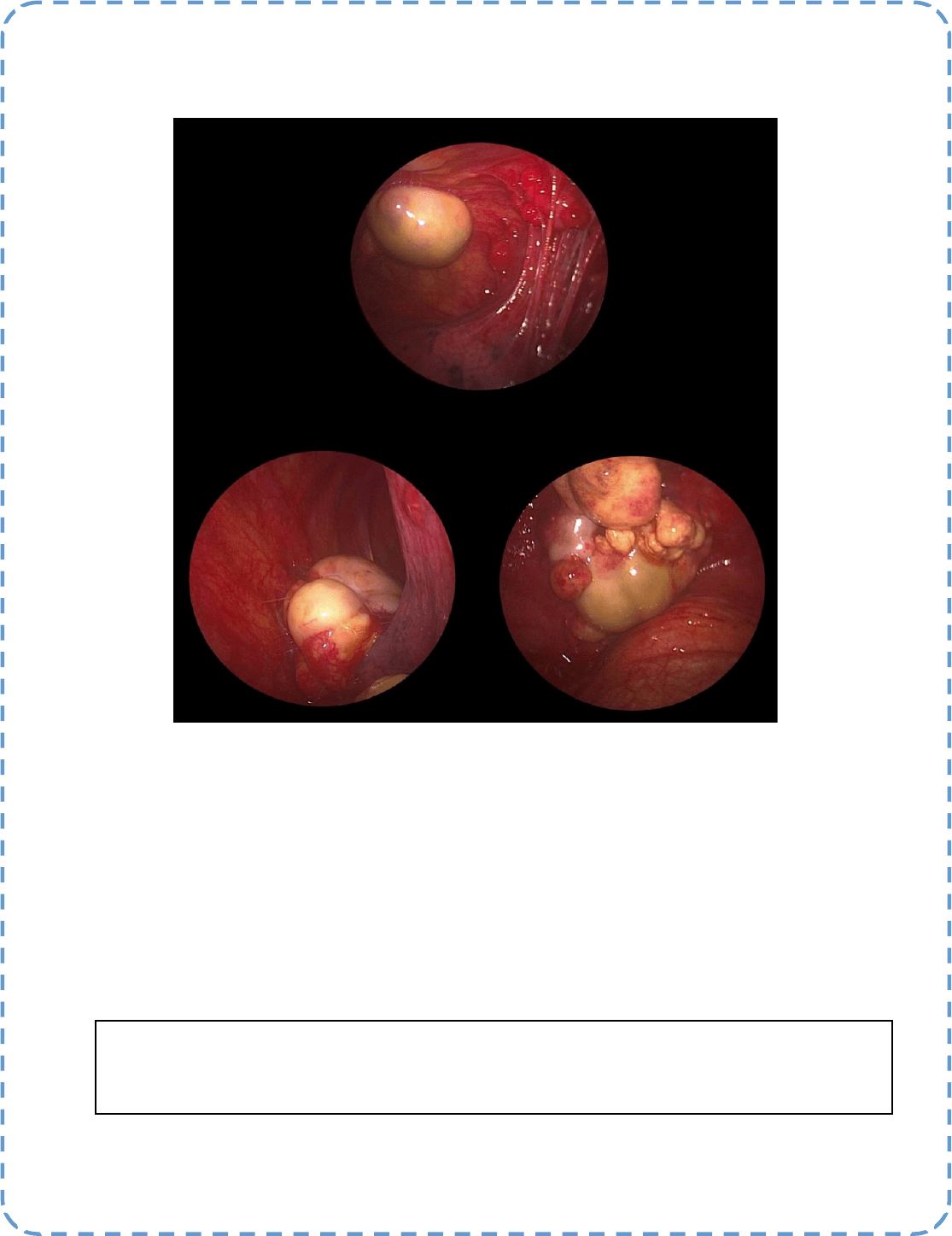
Best Image Contest 2024 (1 of 3)
Category: Pleural Diseases
Descripon: RENAL CELL CARCINOMA- METASTASIS TO THE PLEURAL CAVITY
Submier(s): Pree Vidyasagar, Harikishan Gonuguntla, Suhas Dhulipala, Geetha Sekar
Best Image Contest
P A G E 19
This image is 1 of 3 selected among 100+ submissions to our Best Image Contest held in late 2023. Our next
Image Contest will open later this year. We look forward to receiving your image submissions.

P A G E 20
WABIP News
Highlights of WCBIP/
WCBE Congress 2022
Marseille, France during
the X Paraguayan Con-
gress of Pneumology 2023
On October 25, 2023 the presentaon of the
highlights of the WCBIP MARSELLE 2022 was
held in Paraguay during the X Paraguayan
Congress of Pneumology 2023.
We had the pleasure of having an interna-
onal speaker Dr. Mohammed Munavvar who presented Pre-Congress
Course "Hands-on Intervenonal Bronchoscopy Workshop Course", which
was coordinated by the Naonal Regents Dr. Adid Aluan (current) and Dr.
Domingo Perez (former) of the WABIP (World Associaon for Bronchology
and Intervenonal Pulmonology).
We appreciate the support of these internaonal organizaons for the
collaborave scienc acvity, extending our thanks to the regents of
Argenna on behalf of Dr. Agusn Buero and Dr. Silvia Quadrelli with the
aim of solidifying the pulmonary intervenonalism and thereby increase
the quality of paent care in Lan America.
Call for Abstracts - WCBIP Bali Indonesia 2024
We are excited to receive your abstracts for our com-
ing World Congress. Researchers and professionals in
bronchoscopy and intervenonal pulmonology com-
munity are welcome to contribute original abstracts
in the following areas:
Intervenonal Pulmonology, Laryngology, Pleural,
Tracheobronchology, Throracic Surgery, Esophagolo-
gy,
Intrathoracic Cancer, Pediatric Intervenonal Pulmo-
nology
hps://wcbip2024.com/abstract
Submit your abstracts by May 1, 2024
Cooking Lung Cancer!
Transbronchial Microwave Ablaon of Peripheral Lung Tumors
The exploraon and development of Transbronchial Microwave Ablaon (TBMA) for lung cancer treatment have been driven by several factors.
The increasing availability of CT scans and evidence supporng low-dose CT screening in high-risk populaons have led to the incidental discovery
of small lung nodules, many of which may be premalignant or early-stage tumors. This has emphasized the need for local treatment of these early-
stage lung cancers and oligometastases, parcularly in paents unt for surgery. Tradional thermal ablaon methods, such as radiofrequency
ablaon, carried risks like pneumothorax, bronchopleural stula, and tumor seeding. Microwave energy, less aected by lung ssue impedance,
creates a larger, more predictable ablaon zone, making TBMA a promising alternave.
TBMA combines the benets of microwave energy with a transbronchial approach to avoid pleural puncture and reach lung regions dicult for
percutaneous routes. It uses electromagnec navigaon bronchoscopy for navigaon and cone-beam CT for accurate determinaon of the ablaon
zone. The technique has shown a high technical success rate, short hospital stays, and low complicaon rates. However, TBMA is not without limi-
taons, such as risks associated with nodule size and locaon, requiring careful case selecon.
Future direcons of TBMA include using mobile C-arm machines for 3D reconstrucons, making TBMA feasible outside of hybrid operang rooms.
Advancements in roboc bronchoscopy are also paving the way for easier, more intuive TBMA approaches. Invesgaons into other energy
forms, such as thermal vapor and pulsed electric eld, are ongoing. TBMA, along with these adjuncts, represents an excing development in the
treatment of lung cancer.
The NAVABLATE study was designed to invesgate transbronchial MWA as a minimally invasive treatment opon for lung cancer paents ineligible
for tradional surgery or stereotacc body radiaon therapy(1).
Editor-in-Chief: Dr. Kazuhiro Yasufuku
Research
Primary Business Address:
Kazuhiro Yasufuku, Editor-in-Chief WABIP
Newsleer
c/o Judy McConnell
200 Elizabeth St, 9N-957
Toronto, ON M5G 2C4 Canada
E-mail: newsleer@wabip.com
P A G E 21
Associate editor:
Dr. Ali Musani
Associate editor:
Dr. Sepmiu Murgu
Uzair Ghori MD
Assistant Professor of Medicine,
Medical College of WI,
Medical College of Wisconsin/ VA
Milwaukee
Ali I. Musani MD, FCCP
Professor of Medicine and Surgery,
University of Colorado School of
Medicine, Denver
Conducted in two centers in the UK and China, the study enrolled 30 subjects with lung malignancies, 66.7% of which were primary lung can-
cers and 33.3% oligometastac. The mean age of parcipants was 68.4 years, with 40% female representaon. A striking aspect of the study
was its inclusivity, as 47% of parcipants were not candidates for surgery or SBRT, with others declining these opons.
The technical success of the procedure was outstanding, with a 100% success rate in reaching and ablang targeted nodules. Furthermore,
the one-month post-procedure imaging showed 100% technique ecacy, with no new metastac disease or lymphadenopathy observed.
These results are parcularly encouraging, considering the mean nodule size was 13.7 mm.
In terms of safety, the NAVABLATE study demonstrated a low adverse event rate. Only 3.3% of parcipants experienced mild hemoptysis,
and there were no incidences of pneumothorax or deaths. Addionally, 13.3% experienced grade 3 complicaons, but no higher-grade com-
plicaons were observed.
Paents reported minimal pain and discomfort post-procedure, with a signicant decrease in reported pain over a one-month period. This
was paralleled by a slight improvement in the overall health assessment of parcipants, as measured by the EQ-5D-3L scale.
The NAVABLATE study signies a major leap in lung cancer treatment, establishing transbronchial MWA as a viable, less invasive alternave.
Its high success rate and minimal complicaons mark it as a potenal game-changer for paents with limited treatment opons. The results
pave the way for future studies and the potenal widespread adopon of this technique(2).
References:
1. Lau KKW et al. [published online ahead of print, 2023 Sep 25]. J Bronchology Interv Pulmonol. 2023;10.1097/LBR.0000000000000950. doi:10.1097/
LBR.0000000000000950
2. Chan JWY et al. Cancers (Basel). 2023;15(4):1068. Published 2023 Feb 8. doi:10.3390/cancers15041068
Research
P A G E 22
P A G E
23
WABIP ACADEMY- WEBCASTS
The WABIP has started a new educaon project recently: THE WABIP ACADEMY. The WABIP Academy will pro-
vide free online webcasts with new and hot topics that will interest pulmonologists and intervenonalists.
Current webcast topic: Tissue acquision for biomarker directed therapy of NSCLC
You can reach these webcasts by using this link: hp://www.wabipacademy.com/webcast/
www.bronchology.com Home of the Journal of Bronchology
www.bronchoscopy.org Internaonal educaonal website for
bronchoscopy training with u-tube and
facebook interfaces, numerous teachiing
videos, and step by step tesng and assess
ment tools
www.aabronchology.org American Associaon for Bronchology and I
ntervenonal Pulmonology (AABIP)
www.eabip.org European Associaon for Bronchology and
Intervenonal Pulmonology
W A B I P N E W S L E T T E R
Links
www.chestnet.org Intervenonal Chest/Diagnosc Procedures (IC/DP)
NetWork
www.thoracic.org American Thoracic Society
www.ctsnet.org The leading online resource of educaonal and
scienc research informaon for cardiothoracic
surgeons.
www.jrs.or.jp The Japanese Respirology Society
sites.google.com/site/asendoscopiarespiratoria/
Asociación Sudamericana de Endoscopía Respiratoria
P A G E 23