Volume 10
Issue 03
September 2022
Inside This Issue
Editorial, 2-3
Technology Corner, 4-5
Tips from the Experts, 6-7
Humanitarian News, 8-11
Best Image Contest, 12
WABIP News, 13-14
Research, 15-16
Links, 17
Diagnostic Yield: Apples, Oranges, and Paradigm
Incommensurability
WABIP Newsletter
S E P T E M B E R 2 0 2 2 V O L U M E 1 0 , I S S U E 3
EXECUTIVE BOARD
Hideo Saka, MD
Japan, Chair
Stefano Gasparini,
MD
Italy, Vice-Chair
Silvia Quadrelli, MD
Argenna, Immediate
Past-Chair
David Fielding MD
Australia, Treasurer
Naofumi Shinagawa,
MD
Japan,
Secretary General
Philippe Astoul, MD
France, President
WCBIP 2022
Menaldi Rasmin, MD
Indonesia, President
WCBIP 2024
STAFF
Michael Mendoza
General Manager
Judy McConnell
Administrator
Kazuhiro Yasufuku
Newsleer Editor-in-
chief
P A G E 2
In the past two decades, unprecedented advances in
technology have led to the commercializaon of
new bronchoscopy plaorms which have been wide-
ly adopted as standard of care procedures by inter-
venonal pulmonologists around the globe. In the
US and in Europe, these novel medical devices were
cleared by regulatory stakeholders in the absence of
comparave eecveness studies, based on the
assumpon that similaries in form and funcon to
already available devices obviated the need for such
data. Thus, most studies published to date reporng
on the diagnosc test performance of these novel
devices have been single-arm observaonal studies
using the surrogate endpoint of diagnosc yield
(DY). (1)However, DY captures more than the tech-
nical ability of these devices to navigate to the tar-
geted lesion, and is aected by many other relevant
variables, which include targeted nodule characteris-
cs, operator skills and cancer prevalence, among
others. Perhaps more importantly, DY has been de-
ned in many dierent ways in studies published to
date which further complicate comparisons across
single-arm studies.
Diagnosc yield (DY) is strictly dened as the likeli-
hood that a biopsy will provide a histopathological
diagnosis sucient to guide management with con-
dence. Typically, this would include malignant diag-
noses, usually, although not always, uncontroversial,
and benign diagnoses deemed specic enough to
convince the pathologist that the lesion in queson
was indeed adequately sampled. These would in-
clude granulomatous inammaon, robust neutro-
philic inltraon, or hamartomas among others.
Diagnosc yield is oen confused with diagnosc
accuracy, which represents the degree to which histopatho-
logical diagnosis reects the ground truth.(2) Inammaon,
while non-specic and thus excluded from the prior deni-
on, could in fact represent lesional ssue, but oen re-
main inconclusive at the me of diagnosis, leading to subse-
quent intervenons. Thus, diagnosc accuracy requires
sucient clinical follow-up to adjudicate non-specic be-
nign diagnoses. Studies on diagnosc test performance of
bronchoscopy have oen conated these two noons and
used them interchangeably, leading to incommensurable
esmates of diagnosc test performance even when ac-
counng for dierences in paent populaon. We have
been comparing apples to oranges.
The impact of these dierent denions on DY was recently
evaluated in a Monte-Carlo simulaon by Vachani and col-
leagues. In “The Impact of Alternave Approaches to Diag-
nosc Yield Calculaon in Studies of Bronchoscopy”, pub-
lished in CHEST in 2022, a hypothecal cohort of 1000 pa-
ents undergoing diagnosc bronchoscopy was assessed
using 3 commonly used but disnct methods for DY calcula-
on: (1) a strict approach, which corresponds to actual DY
as dened above, (2) an intermediate approach, in which
non-specic benign diagnoses were considered diagnosc if
clinical follow-up did not reveal malignancy, and (3) a liberal
approach, according to which even non-diagnosc samples
(such as normal lung or pleura) were considered diagnosc
if follow-up did not reveal malignancy. Expectedly, es-
mates of “DY” varied considerably, ranging from 67% to
88%, a 21% absolute dierence simply due to an arbitrarily
chosen method of reporng the data.(3)
The implicaon of these observaons is obvious: studies
using dierent denions of DY are dicult, if not impossi-
ble to compare. Denions of DY should be explicitly and
Crisna D. Salmon, MD
Department of Allergy, Pulmonary and
Crical Care Medicine,
Vanderbilt University Medical Center
Fabien Maldonado, MD, MSc
Department of Allergy, Pulmonary and
Crical Care Medicine,
Vanderbilt University Medical Center
W A B I P N E W S L E T T E R
P A G E 3
the proper conduct of methodologically sound comparave
studies, with randomized controlled trials standing rm as the
pinnacle of comparave eecveness research, uniquely able
to account for both known, and unknown confounders.
References
1. Agrawal A et al. Ann Thorac Surg. 2022 Jan 17;S0003-4975
(22)00042-X.
2. Baratloo A et al. Emerg Tehran Iran. 2015;3(2):48–9.
3. Vachani A et al. Chest. 2022 May;161(5):1426–8.
4. Folch EE et al. J Thorac Oncol O Publ Int Assoc Study Lung
Cancer. 2019 Mar;14(3):445–58.
transparently reported, with data available to allow
reviewers and readers to re-calculate DY based on
their preferred approach. While we do not recom-
mend one method over another, we suggest that
the liberal method be abandoned, as it is most like-
ly to be inuenced by cancer prevalence: for exam-
ple, with a 10% cancer prevalence in the popula-
on studied, the esmate of DY will approach 90%
even if most lesions are missed. Unfortunately, this
method has been the tradional method used in
the bronchoscopy literature unl recently.(4) More
fundamentally, even if the enre bronchoscopy
community was to uniformly agree on a DY deni-
on, variaons in cancer prevalence, nodule char-
acteriscs, operator skillset and biopsy tools used
would sll aect esmates of DY independently of
the actual technical ability of the bronchoscopy
plaorm. Thus, DY should be regarded as a surro-
gate for diagnosc test performance, more accu-
rate esmates of which may only emerge through
W A B I P N E W S L E T T E R
P A G E 4
Technology Corner
Endobronchial Ultrasound-Guided Radiofrequency Ablaon for Lung Cancer
INTRODUCTION
Transbronchial ablaon therapy has been evaluated to reduce the high rate of complicaons associated with percutaneous ablaon
for lung cancer.
1-5
Although there is limited clinical evidence for transbronchial ablaon, preliminary data suggests it has a beer
safety prole than percutaneous ablaon.
3,4
One major challenge with transbronchial ablaon is the placement of the electrodes,
parcularly when there is no single bronchus leading to the tumor (negave bronchus sign).
6
BACKGROUND
Olympus Corporaon developed a needle-type (19 gauge) bipolar radiofrequency ablaon (RFA) device that is compable with cur-
rent convex-probe EBUS bronchoscopes. The needle’s distal poron serves as an electrode and is echogenic for easier ultrasound
visibility. Once the needle is inside the targeted nodule, a second electrode is deployed from the p. In animal models, we evaluated
the safety of EBUS-guided RFA, as well as the correlaon between energy delivery and ablaon extent.
7
Room-temperature saline
was connuously injected throughout the ablaon at a predetermined rate via an integrated infusion channel to enhance electrical
conducvity. Promising safety and ecacy data prompted a clinical pilot study of EBUS-guided RFA.
8
CLINICAL APPLICATION
Study design
A prospecve, single-arm, ablate-and arm, ablate-and-resect trial (ClinicalTrials.gov, NCT03400748) was conducted at Toronto Gen-
eral Hospital (Toronto, Canada). The primary outcome of this pilot study was short-term safety. Immediately following RFA, resec-
on was performed to assess the ablated area histologically, including adjacent healthy peritumoral ssue. Adult paents aged 18
and older who had either (1) pathologically proven stage I or stage II lung cancer with a primary tumor larger than 1 cm, or (2) a met-
astac lung nodule larger than 1 cm, and for whom this tumor/nodule was accessible by convex-probe EBUS bronchoscope were
included in this study.
Procedures
The RFA probe was inserted into the target lung nodule under EBUS guidance followed by ablaon with a total supplied energy of 4
to 8 kJ. The total energy was purposefully determined to avoid complete tumor ablaon, as the objecve of this study was to evalu-
ate the short-term safety of EBUS-guided RFA. During RFA, the posion of the electrodes was monitored using cone-beam CT uor-
oscopy. Aer EBUS-guided RFA, bronchoscopy and a contrast CT were performed to document o-target injuries. Following the ac-
quision of all images, the paent had surgical resecon in the same operang room under the same anesthec.
Tsukasa Ishiwata, MD, PhD
University Health
Network
Alexander Gregor, MD
University Health
Network
Kazuhiro Yasufuku MD, PhD
University Health
Network
W A B I P N E W S L E T T E R
P A G E 5
Study results
In ve dierent individuals, ve primary lung malignancies were ablated (adenocarcinoma in four cases, squamous cell carcinoma in
one case). For 4 kJ, 6 kJ, and 8 kJ, the mean ablaon mes were 13.8 min, 8.4 min, and 15.6 min, respecvely. Throughout the RFA
procedure, the posion of the RFA device was connuously monitored and veried within the target using EBUS. The average proce-
dure me was 36.2 min (range, 26-51 min). There were no signicant immediate complicaons related to EBUS-guided RFA. Parcu-
larly, neither during inseron, deployment of the second electrode, nor ablaon was there any major hemorrhage that required for
intervenon. On post-RFA bronchoscopic examinaon, there was no evidence of thermal injury to the bronchial wall. The post-RFA
contrast CT revealed no pneumothorax or hemothorax.
Advantages
As the RFA probe does not pass through the pleura, the transbronchial approach naturally has a lower risk of pneumothorax than the
transthoracic approach. Doppler mode EBUS can help avoid intervening vessels, which may lower the risk of bleeding or development
of bronchovascular stulas. The study design did not allow evaluaon for late sequelae of bronchial thermal injury; however, the ab-
sence of acute injury is reassuring. This technique's ulmate goal is to treat lung tumors in the middle- and central-third lung elds.
The current 6.9 mm-EBUS bronchoscope has limited access to lung lesions not adjacent to the central airways. It will probably be nec-
essary to combine EBUS-guided RFA with a thin EBUS bronchoscope to improve access to the periphery. Our team has published the
performance of a prototype thin bronchoscope (distal end outer diameter: 5.9 mm), showing noceably enhanced access to the sub-
lobar bronchi.
9
Transbronchial RFA in the middle lung eld may have even further advantages over central RFA. This includes poten-
al improvements in safety (greater distance from the heart, large vessels, central airway, and esophagus) and ecacy (reduced heat
sink eect due to decreased vessel diameter in the lung periphery).
CONCLUSION
This pilot study showed that EBUS-guided RFA may access lung tumors close to airways, enabling real-me monitoring of the elec-
trode deployment and ablaon with no immediate complicaons. EBUS-guided ablaon may avoid some of the morbidity of percuta-
neous ablaon.
References
1. Tsushima K et al. Eur Respir J. 2007;29:1193-200.
2. Suzuki H et al. J Bronchology Interv Pulmonol. 2011;18:211-7.
3. Koizumi T et al. Case Rep Oncol Med. 2013;2013:515160.
4. Xie F et al. Respiraon. 2017;94:293-8.
5. Sa S et al. Lung Cancer. 2018;124:125-9.
6. Tsuboi E et al. Cancer. 1967;20:687-98.
7. Motooka Y et al. Semin Thorac Cardiovasc Surg. 2020;32:570-8.
8. Ishiwata T et al. J Thorac Cardiovasc Surg. 2022; 164(4):1188-
1197
9. Ishiwata T et al. Transl Lung Cancer Res. 2022;11:1292-301.
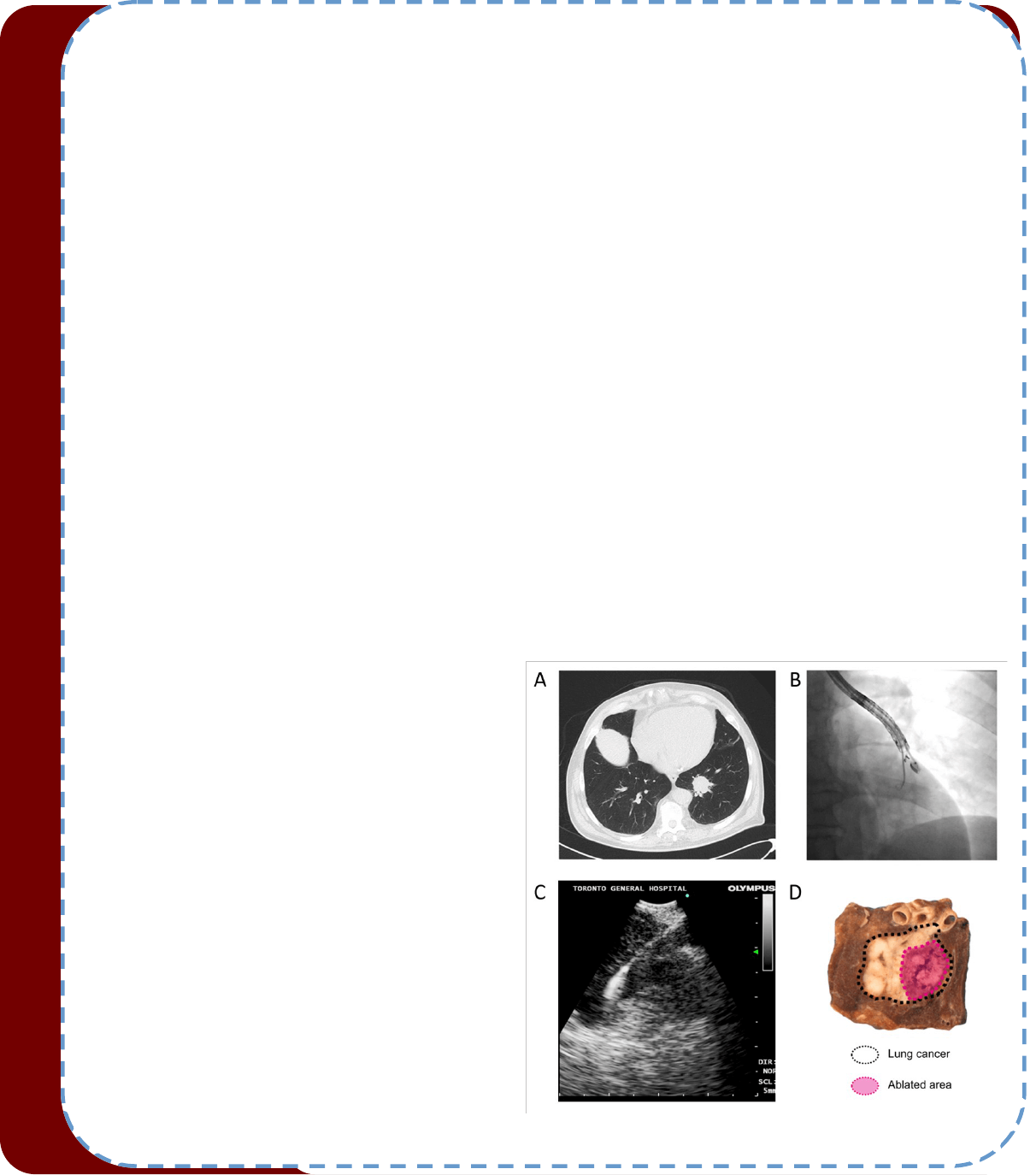
Figure: A representave case of EBUS-guided RFA. (A) A pre-
RFA CT axial view (71-year-old male with stage IB squamous
cell carcinoma. (B) Fluoroscopic conrmaon of the elec-
trode posion. (C) An EBUS image before ablaon. The RFA
electrode was connuously observed throughout the abla-
on. (D) Gross pathological examinaon of the resected
specimen.

Tips from the Experts
P A G E 6 V O L U M E 1 0 , I S S U E 3
Introducon
Endobronchial ultrasound transbronchial needle aspiraon (EBUS-TBNA) has an excellent diagnosc yield for primary pulmonary malignan-
cies, but the amount of ssue might be insucient to allow for a rm diagnosis of lymphoproliferave disorders or even sarcoidosis. These
enes, especially lymphomas, require histopathologic rather than cytologic samples for the evaluaon of the overall background architec-
ture and correct subtyping (1). Cryobiopsy is an endoscopic technique mostly used in the diagnosc approach to intersal lung disease,
based on rapid cooling, crystallizaon, and subsequent collecon of ssue. Herein we share our approach in performing EBUS-TBNA and
transbronchial mediasnal cryobiopsy (TMC) during the same procedure for diagnosc purposes of mediasnal lesions and lymph nodes.
Indicaons
1. Proven or suspected malignancy, either of solid or hematologic origin and sarcoid suspicion.
2. Mediasnal lymph nodes with diameter ≥ 1 cm in the short axis.
3. Paents with at least one mediasnal/hilar lesion irrespecve of the lymph node staon.
4. Necessity to undergo endoscopic mediasnal assessment for diagnosis, staging or molecular characterizaon.
5. Paents with previous non diagnosc EBUS-TBNA.
Planning
The planning for performing a TMC begins with the CT or PET-CT images. If it´s a diagnosc procedure, and feasible, we recommend se-
lecng the hilar staons rst; in our experience the 1.1 mm cryo-probe (Erbecryo 20402-401, Tubingen, Germany) enters these areas more
smoothly than the mediasnal ones. It is important to idenfy the lymph node staons that are closest to the bronchial or tracheal wall,
since those that are further away will be more dicult to access with the cryoprobe, making the procedure longer and more complex.
Sampling and Procedure
We perform the procedure under conscious (moderate) sedaon. Herein we describe the step-by-step approach applying our method (2)
through a clinical case descripon. A 42-year-old female was referred to our Intervenonal Pulmonology Unit (IPU) due to enlarged medias-
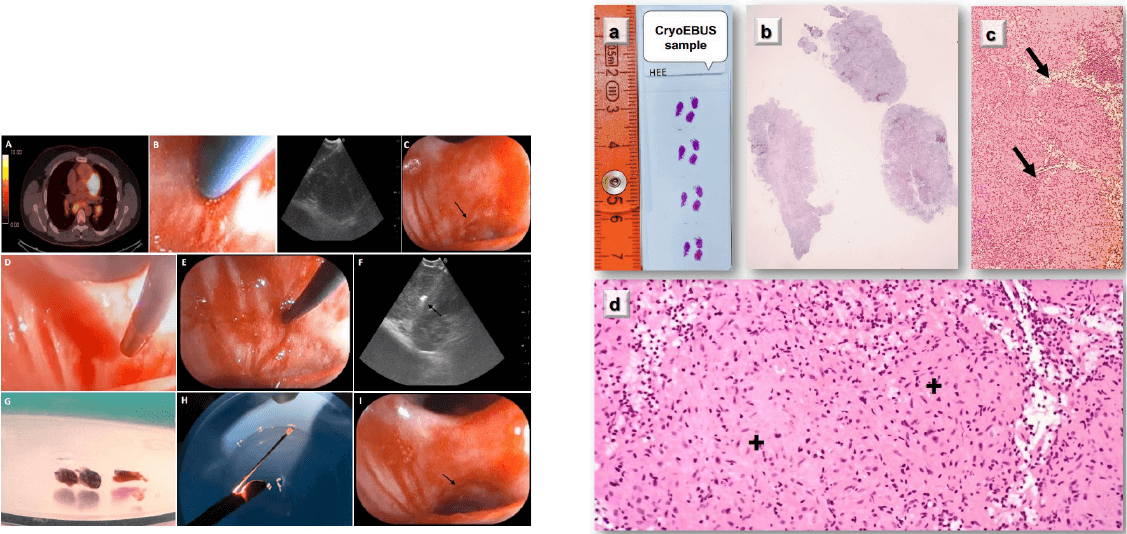
nal and hilar lymph nodes. The PET-CT scan showed an increased FDG uptake at staons 7 and 11L (Figure 1A). Aer idencaon of an
enlarged staon 7 lymph node on EBUS (Pentax Medical EB19-J10U), we performed three passes of TBNAs with 22-gauge needle
(SonoTip
®
TopGain: Medi-Globe) (Figure 1B). Aer inial puncture with the TBNA needle, a 1.1 mm cryo-probe was introduced into the work-
ing channel of the EBUS bronchoscope. The cryo-probe is advanced towards the puncture site and inserted gently through the previous
puncture site created by the TBNA needle. The EBUS image conrmed the cryo-probe posion within the lymph node. The cryo-probe was
cooled down for 4 s, and then retracted with the bronchoscope and the frozen biopsy ssue aached to the p of the probe (Figure 1C-G).
The cryobiopsy site was immediately examined and no bleeding was observed (Figure 1H). Cryobiopsies were retrieved in saline and xed in
formalin (Figure 1I). Samples conrmed the diagnosis of sarcoidosis (Figure 2).
EBUS-GUIDED TRANSBRONCHIAL MEDIASTINAL CRYOBIOPSY
Javier Pérez Pallarés
Intervenonal Pulmonologist
Cartagena Hospital, Spain
Miguel Ariza Prota, MD
Intervenonal Pulmonologist
Asturias Central University Hospital, Spain
Rosa Cordovilla, MD, PhD
Director of Intervenonal Pulmonology Unit
Salamanca University Hospital, Spain
Tips from the Experts
P A G E 7 V O L U M E 1 0 , I S S U E 3
Quality Control
It is important to menon that our method for performing TMC is mainly based on always introducing the cryoprobe under ultrasound guid-
ance; we do not focus on trying to introduce the cryoprobe through the puncture site only. We are guided by the track le in the lymph node
by EBUS-TBNA needle. It is key to introduce the cryoprobe at the same angle in which the previous EBUS-TBNA punctures were performed.
Every me we obtain a TMC, we immediately return with the EBUS to the punctured staon and spend ~ 2 min visualizing its ultrasonograph-
ic characterisc under Doppler mode, looking for signs of bleeding within the lymph node.
Zhang et al. conducted a trial that included a total of 197 paents who underwent EBUS-TBNA and TMC in the same procedure to assess the
diagnosc yield and safety of this technique. For TMC they performed a small incision in the tracheobronchial wall adjacent to the medias-
nal lesion using a high-frequency needle-knife (3). An important dierence in our method is the way we perform the procedure. We have
shown that the high-frequency needle knife is not essenal, and we eliminated this step of the process by directly introducing the 1.1 mm
cryo-probe always under echo guidance through the puncture site created by the EBUS-TBNA needle. This modied technique allows us to
perform the procedure in a faster and less invasive way. Prior studies reported an intranodal forceps biopsy (IFB) strategy for mediasnal
lesions, which emphasizes the essenality of sample amount for improving diagnosc sensivity (4). Agrawal et al. performed a meta-analysis
and concluded that the addion of EBUS-IFB to EBUS-TBNA improves the overall diagnosc yield of sampling intrathoracic adenopathy when
compared with EBUS-TBNA alone. The complicaon rates of the combined approach were higher than with EBUS-TBNA (5). In our pracce,
TMC does not have greater complicaons than EBUS-TBNA. It would be interesng to compare the diagnosc yield and complicaons be-
tween TMC and IFB in the future.
Conclusion
We believe EBUS-guided TMC, compared to EBUS-TBNA, provides more adequate histological samples, adding value to current diagnosc
approaches for mediasnal diseases, especially for lymphoproliferave disorders, or when more ssue is needed for molecular determina-
ons. Further studies are needed to address safety and outcomes of this technique.
References:
1. Franke K et al. Lung. 2012;190:227–32.
2. Ariza M et al. Arch Bronconeumol. 2022 May 30:S0300-2896(22)00390-8.
3. Zhang J et al. Eur Respir J. 2021;58:2100055.
4. Herth F et al. Ann Thorac Surg. 2008 Jun;85(6):1874-8.
5. Agrawal A et al. Ann Thorac Surg. 2022 Jul;114(1):340-348.
Figure 1. PET-CT scan showed an increased FDG uptake at staons 7 and
11L (A). Performing EBUS-TBNA in staon 7; TBNA needle sheath (B). Punc-
ture site made by TBNA needle, black arrow (C). Tip of the cryo-probe ap-
proaching the puncture site (D), and a p of the cryo-probe completely
inside the node (E). EBUS image showing the p cryo-probe within the
lymph node, black arrow (F). Tip of the probe has the lymph node ssue
obtained by cryo-nodal biopsy (G). Bronchoscopic view of the puncture site
aer performing cryo-nodal biopsy, black arrow (H). Samples obtained
from transbronchial mediasnal cryobiopsy (I).
Figure 2. Gross-micro view of the cryobiopsy specimen, with 0.5 cm
fragments (A-B). Histological secon (H&E). Hypercellular areas orga-
nized in nodules are observed (arrows). No necrosis (C). Nodular areas
composed of epithelioid cells clusters (+), forming granulomas. Non-
necrozing granulomatous lymphadenis, compable with sarcoido-
sis (D).
Humanitarian News
W A B I P N E W S L E T T E R P A G E 8
WABIP’s Instute of Intervenonal Pulmonology
Wrien by Ali I. Musani
The World Associaon for Bronchology and intervenonal Pulmonology (WABIP) has come a long way since its incepon,
parcularly in the last decade. The membership has grown steadily over the years to almost 10 thousand. The educaonal,
philanthropic, and social endeavors have expanded at an impressive pace. WABIP has shown remarkable progress, and its
leadership should be proud of these achievements.
Focusing on our organizaon's fundamental goals and concerted eorts to achieve them is vital. WABIP's goals, as outlined
in the mission and goal statement of the WABIP, are "to strengthen global es between regional and naonal sociees or
groups from around the world to enhance paent care, research, and educaon in bronchology and related elds."
I rmly believe that we are at an inecon point in our society's history to do something far beyond what we have done.
With our thousands of experts worldwide, access to rapidly developing and state-of-the-art technologies, close relaonship
with industry, and our unied mission across connents, we have an enormous potenal to do great things for the dissemi-
naon of science and the eld of Intervenonal Pulmonology. We can genuinely democraze the eld of Bronchology and
Intervenonal Pulmonology and eventually disseminate the knowledge, skills, and technology to improve paent care across
the globe. We desperately need to blur the line between resource-poor and resource-rich areas worldwide. Those lines are
men made, aer all.
I have a dream!
WABIP Intervenonal Pulmonology Instute (IPI)
For the last ten years, I have been quietly exploring locaons, business models, educaonal structure, organizaonal feasibil-
ity, and other aspects of developing several instutes of Intervenonal Pulmonology around the globe. I have had signicant
breakthroughs in the last three years, rst in Kuala Lumpur, Malaysia, and then in Istanbul, Turkey.
Both sites have most, if not all, the prerequisites for a fantasc training site for doctors from around the world regardless of
their country of origin, nancial, and social background. We (local IP leaders in Malaysia, Turkey, and me) have had numer-
ous meengs with the leadership of both instuons. We have developed a memorandum of understanding (MoU) and ne-
goated the basic tenets of our partnerships. We presented the progress report of our potenal collaboraon to the board
of directors and the board of regents of the WABIP. The project received overwhelming support, ocial approval, and nan-
cial support from the execuve board of the WABIP to move forward. I have accepted the honor of chairing the ad hoc com-
miee of the WABIP for the development of IPI and formed mulple commiees to achieve these projects' administrave
and educaonal goals. Fundamentally, the IPI will have a mulfaceted educaon, training, technology transfer, and research
mission. Please see below for the details.
IPI Concept:
WABIP will collaborate with public and private hospitals and local IP experts aliated with WABIP around the world. In part-
nership with the host hospital, WABIP will set up Instutes of Intervenonal Pulmonology to oer IP educaon and training
for doctors worldwide and IP-related health services to regional paents.
The host hospital will provide:
• The host hospital will provide the infrastructure for educaon, training, and health care delivery, including a facility
equipped with operang rooms, bronchoscopy suite, pre and post-operave areas, a clinic, an oce, a conference room,
and an in-paent facility.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 9
• The host hospital will provide devices necessary for training IP and paent care, such as exible and rigid bronchoscopes,
Endobronchial Ultrasound (EBUS), Radial ultrasound (REBUS), Navigaon bronchoscopy system, pleuroscope, airway stents,
laser, and electrocautery.
• The host hospital will also provide nancial support for the educaonal program, including airfare, transportaon, resi-
dence, and food for up to 24 faculty (provided by the WABIP) per year.
• The host hospital will arrange malpracce insurance for the faculty.
• The host hospital will aid in obtaining a short-term medical license without going through extensive tesng or documenta-
on from the local government to allow WABIP physicians and trainees to perform procedures on local paents.
• WABIP and the host hospital will seek funding from philanthropic organizaons, individuals, and industry to support the
mission of IPI. They will also collect device donaons (new, used, or refurbished) from industry and hospitals in the resource-
rich parts of the world.
WABIP will provide:
• Expert faculty for teaching and training as well as for performing state-of-the-art procedures on the local paents
• Curriculum and training infrastructure for IP fellowship/mini-fellowship/training for the internaonal trainees
• The Fellowship commiee will screen, invite, train, and cerfy internaonal doctors in dierent disciplines of the IP
WABIP Fellowship:
The fellowship commiee comprised of world experts of IP educators will develop fellowships in specic IP-related areas
such as advanced diagnosc bronchoscopy (including EBUS, Radial EBUS, peripheral bronchoscopy), therapeuc bronchosco-
py (including rigid bronchoscopy, ablaon, and airway stenng), and Pleurology (including pleural procedures). They will
develop policies and processes for selecng fellowship applicants, curriculum, create or use already established standardized
educaonal tools and training methods, and cercaon processes. A cered fellow from WABIP IPI will be able to start an
IP program in their country and train others aer a necessary period of pracce.
WABIP will strive to train fellows who would be able to set up IP programs in their countries with their personal/naonal or
WABIP resources and teach more people and open more centers in the region (the trickle-down eect)
Where are we now?
We selected the rst partner site with the help of Dr. Jamalul Azizi in Kuala Lumpur, Malaysia. Dr. Azizi is the Chair of the
Malaysian Associaon of Bronchology and Intervenonal Pulmonology and a well-known naonal and internaonal leader in
IP. The Cardiac Vascular Sentral of Kuala Lumpur (CVSKL) has a state-of-the-art medical facility where Dr. Azizi pracces IP.
We had several meengs with the leadership of CVSKL, including Mr. Khairul Amin Mohd Nordin, Director of the Clinical Ser-
vices Division, Tan Eng Ghee, CEO, and others. Basic MoU has been negoated. We are nalizing some last details and hope
to discuss and complete the legal contract in three to six months.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 10
Meengs between the IPI (WABIP) leadership and Cardiac Vascular Sentral Kuala Lumpur (CVSKL) leadership.
Top le, Dr. Jamalul Azizi Abdul Rahaman; Top right, Dr. Ali Musani; Middle le, Lim Wang Ying, Head of Health Screening;
Middle right, Tan Eng Ghee, CEO; Boom, Khairul Amin Mohd Nordin, Director of Clinical Services Division
Our second partner site is Liv Hospital Group, Istanbul, Turkey, led by Dr. Levent Dalar.
Dr. Dalar is a well-respected Intervenonal Pulmonologist in Europe. He has served Turkish and the World Associaon of
Bronchology and Intervenonal Pulmonology for several years. I met with the CEO of the Liv Hospitals in Istanbul in Febru-
ary of 2022 and then with the CEO of the enre hospital group mulple mes via zoom. Our progress in Istanbul has been
swi. We have ironed out most of the signicant aspects of our collaboraon through a detailed MoU. The two most rele-
vant areas recently sorted out include medical licenses and malpracce coverage for internaonal physicians. The Turkish
government will allow WABIP faculty to perform procedures for educaonal purposes as a guest lecturer, temporarily ap-
pointed at the İsnye University, the academic partner of the Liv Hospital Group. The fellows will be covered to do proce-
dures under the supervision of the faculty. The hospital will provide malpracce insurance for all faculty and fellows.
Dr. Mehmet Akif Benk, CEO-General Manager Liv hospital Istanbul and Dr. Levent Dalar, Intervenonal Pul-
monologist at Liv hospital, on the right.
Top right, Dr. Levent Dalar; boom right, Meri Isro, CEO of Liv hospital system Turkey.
We are entering the nal stages of the MoU for IPI, aer which we will draw a formal, legally binding contract for both par-
es. We will then put together a list of faculty for each IPI and apply for local approval and malpracce through the respec-
ve hospital/university menoned above. We hope to achieve these by the rst quarter of 2023 and start the programs soon
aer, with an expected ramp-up period of two years. We will be looking for many WABIP faculty to volunteer for teaching
and training at these instutes.
Our industry and markeng eorts have already started. Dr. Dalar and I met with several European device industry repre-
sentaves. The group outlined many areas of collaboraon, including fellowship sponsorships, device donaons, and nan-
Humanitarian News
W A B I P N E W S L E T T E R P A G E 11
cial donaons. We look forward to meeng with a much larger industry liaison group in Marseille during the WCB to launch a
large-scale campaign for IPI.
Aer these two projects are up and running, I want to establish more instutes in North Africa and South America in the
next few years.
*The views expressed in this arcle are those of the author (Ali Musani) and do not necessarily reect the ocial posions of
the Execuve Board or Internaonal Board of Regents of the WABIP.
Best Image Contest 2022 (3 of 3)
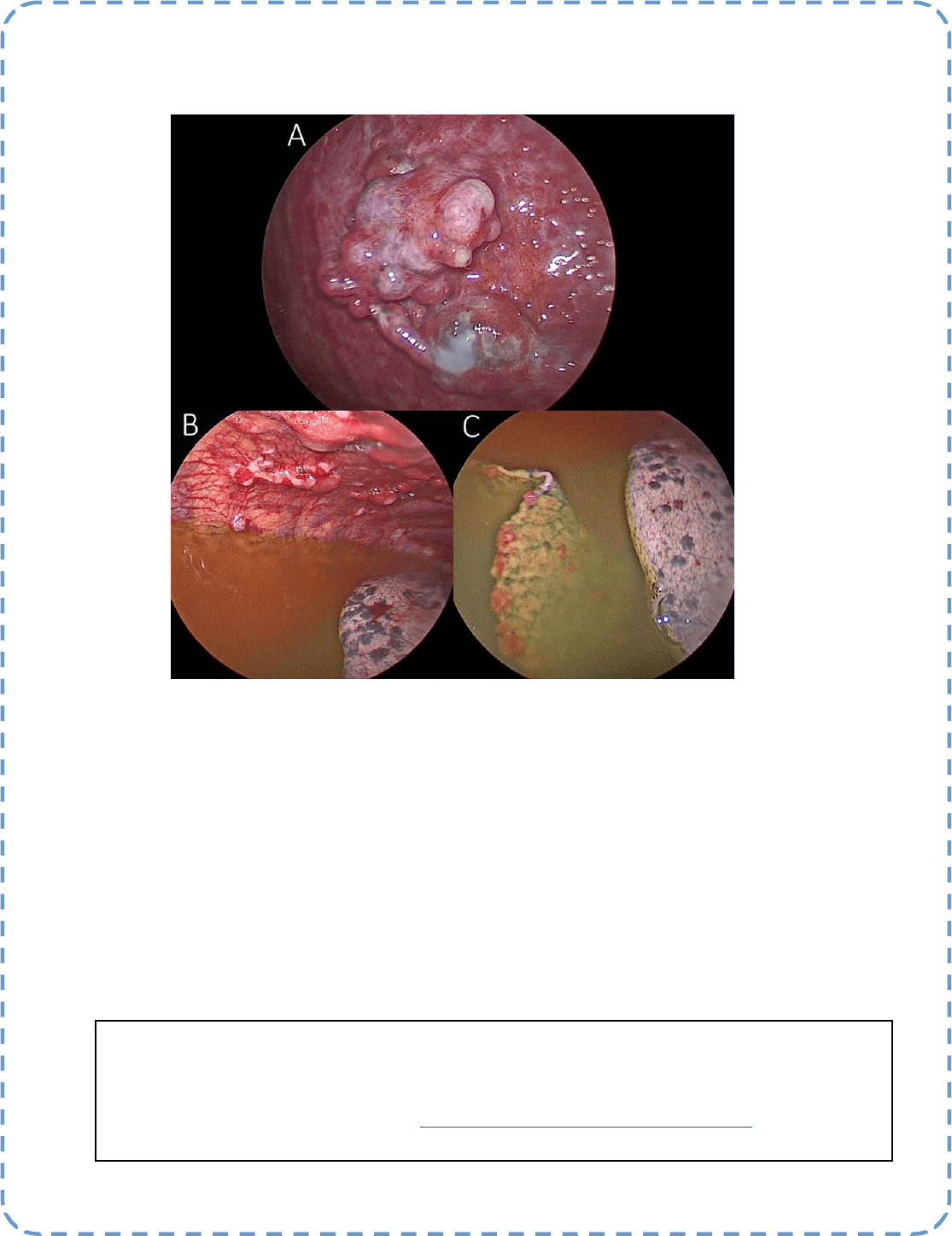
Descripon:
Diuse Malignant Inltraon by Lung Cancer
A: Malignant nodules on the diaphragm, B: Malignant nodules on the parietal pleura, C: Malignant nodules
on visceral pleura
Submiers:
Dr. Pree Vidyasagar, Dr. Hari Kishan Gonuguntla
Best Image Contest
P A G E 12
This image is the 1 of 3 selected among 100+ submissions to our Best Image Contest held in late 2021. Please
stay tuned to the next Image Contest opening later this year. Find the above image and more at the WABIP
Academy Image Library at hps://www.WABIPacademy.com/imagelibrary

P A G E 13
WABIP News
Celebrang the 2022 WABIP Awards
We are happy to announce the results of the 2022 WABIP Awards. The below list of awardees are recognized for
their accomplishments and commitments to bronchology and intervenonal pulmonology, and it is with great
honor to celebrate these recipients at our Awards ceremony of our upcoming WCBIP congress in Marseille
France.
Gustav Killian Centenary Medal 2022 Recipient
Marn Phillips, MD (Australia)
WABIP-Dumon Award 2022 Recipient
Sepmiu Murgu, MD (USA)
WABIP Lifeme Achievement Award 2022 Recipient
Teruomi Miyazawa, MD (Japan)

P A G E 14
WABIP News
Celebrang the 2022 WABIP Awards (cont.)
Disguished WABIP Regent Award 2022 Recipient
Spasoje Popević, MD (Serbia)
Heinrich Becker Young Invesgator Awards for Research and Clinical Innovaon 2022 Recipients:
1. Keisuke Kirita, MD (Japan) for the WCBIP accepted abstract tled:
Development of arcial intelligence system classifying malignant and benign cells for rapid on-site cytologic
evaluaon (ROSE) samples of bronchoscopy
2. Øyvind Ervik, MD (Norway) for the WCBIP accepted abstract tled:
Automac idencaon and segmentaon of mediasnal lymph nodes and blood vessels in endobronchial
ultrasound (EBUS) using a deep neural network
3. Sandip Saha, MD (USA) for the WCBIP accepted abstract tled:
A First for Roboc Navigaonal Bronchoscopy and the Use of “Tele-ROSE” in diagnosing lung pathology
Register for WCBIP Virtual 2022
We are pleased to have already 850 conrmed on-site aendees at our com-
ing WCBIP in Marseille France. This is the perfect opportunity for delegates to
network and learn from some of the top experts in the eld.
If you can't aend in person, you can sll parcipate via Zoom (virtual), as we
will broadcast live selected sessions. Addionally, on-demand playback of all sessions will be available aer the
congress.
• View the Program Schedule Virtual
• View the Program Schedule ALL
• REGISTER HERE
The Devil Is In The Detail
Lung cancer accounts for almost 1.8 million deaths yearly and is responsible for more than 18% of cancer-related mortality worldwide. Lung cancer
is tradionally classied by histology; small-cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC). NSCLC is more common than SCLC and is
further subdivided into squamous and non-squamous categories. Adenocarcinomas constute most non-squamous NSCLC cancers. Tobacco smok-
ing is strongly associated with SCLC and squamous cell carcinoma but remains associated with all histologic subtypes. Recently, a greater under-
standing of disease biology and the idencaon of oncogenic driver alteraons has revoluonized the therapeuc landscape of NSCLC. Conse-
quently, the new classicaon algorithms of NSCLC characterize them molecularly into aconable mutaons with targeted therapies.
Molecular tesng has become a mandatory component of the NSCLC workup. There are almost a dozen NSCLC molecular targets that have ap-
proved therapies. The detecon of EGFR, BRAF, and MET mutaons and ALK, ROS1, RET, and NTRK translocaons is now the standard of care. Tar-
geted therapies for EGFR exon 19 deleon and L858R mutaons and ALK and ROS1 rearrangements are well established. Several other biomarkers,
e.g., KRAS G12C substuons and HER2 acvang alteraons, are becoming mainstream in NSCLC workup with ancipated targeted therapies.
Most centers now rounely perform analysis of PD-L1 protein expression to ulize immune checkpoint inhibitors. The immune checkpoint inhibi-
tors in the NSCLC management also contributed to the signicant improvement of disease outcomes, parcularly in paents lacking TKI-sensizing
mutaons.
Molecular characterizaon of NSCLC requires analysis of biological markers such as DNA, RNA, and proteins, which in turn requires mulple
plaorms such as PCR, FISH, and DNA sequencing. High throughput sequencing technologies such as next-generaon sequencing (NGS) have
served very well in this regard. However, it's me-consuming (10 or more working days) and expensive. Hopefully, this technology will become
Editor-in-Chief: Dr. Kazuhiro Yasufuku
Research
Primary Business Address:
Kazuhiro Yasufuku, Editor-in-Chief WABIP
Newsleer
c/o Judy McConnell
200 Elizabeth St, 9N-957
Toronto, ON M5G 2C4 Canada
E-mail: newsleer@wabip.com
P A G E 15
Associate editor:
Dr. Ali Musani
Associate editor:
Dr. Sepmiu Murgu
Ali I. Musani MD, FCCP
University of Colorado School of Medicine,
Denver
more ecient and cost-eecve.
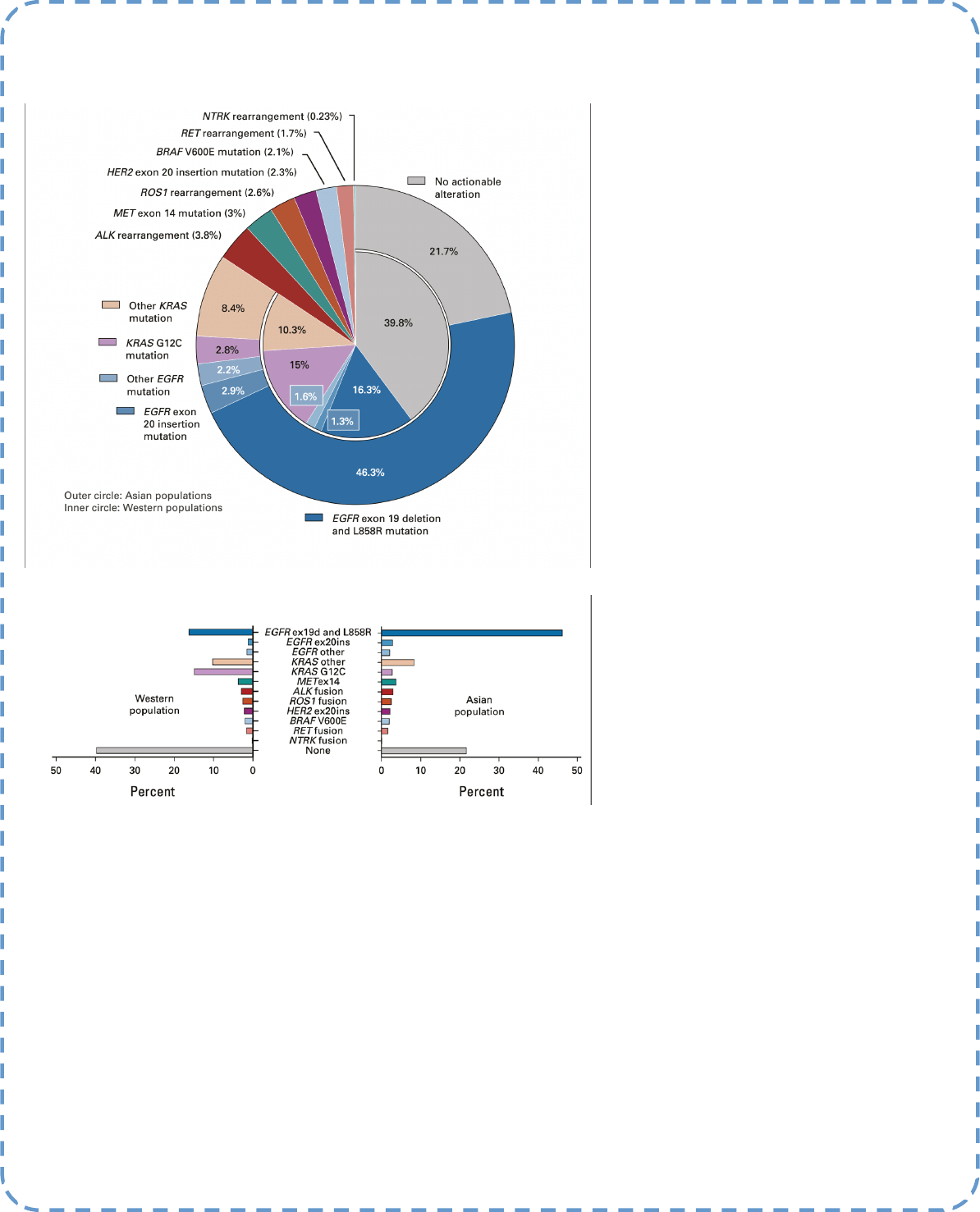
Approximately 50–70 % of Asian and 30–40 % non-Asian NSCLS (non-squamous) paents carry targetable mutaons (g 1) and, when treat-
ed appropriately, show signicantly (several folds) improved survival. Unfortunately, most of this progress has not translated into squamous
cell carcinoma paents. Regardless, the last decade has shown a tremendous improvement in personalized and precision therapy of NSCLC
and is exemplary in medical oncology.
When ssue sampling is not feasible in situaons such as recurrent disease, liquid biopsy can provide important informaon about tumor
evoluon during the treatment course. It does, though, require a high tumor burden. There are assays ulizing circulang tumor cells. How-
ever, it is not clear whether they are representave of the enre tumor or a fracon of heterogeneous cancer. The amount of circulang
tumor DNA correlates with tumor response or lack thereof and can be ulized as a marker of the ecacy of therapy.
The tremendous promise lies in more profound discoveries in tumor biology, broad-based clinical trials, and rapid drug development.
References:
1. Tan AC et al. J Clin Oncol. 2022 Feb 20;40(6):611-625. doi: 10.1200/JCO.21.01626. Epub 2022 Jan 5. PMID: 34985916.
2. Imyanitov E et al. Crit Rev Oncol Hematol.2021 Jan;157:103194
Research
P A G E 16
Figure 1. Frequency of targetable oncogenic driver
molecular alteraons in NSCLC (adenocarcinoma).
Incidences of oncogenic driver alteraons extract-
ed from the studies by Burne et al,Dearden et
al,Jordan et al, Shi et al,and Solomon et al.d, dele-
on; ex, exon; ins, inseron; NSCLC, non–small-cell
lung cancer. (1)
P A G E
17
WABIP ACADEMY- WEBCASTS
The WABIP has started a new educaon project recently: THE WABIP ACADEMY. The WABIP Academy will pro-
vide free online webcasts with new and hot topics that will interest pulmonologists and intervenonalists.
Current webcast topic: Tissue acquision for biomarker directed therapy of NSCLC
You can reach these webcasts by using this link: hp://www.wabipacademy.com/webcast/
www.bronchology.com Home of the Journal of Bronchology
www.bronchoscopy.org Internaonal educaonal website for
bronchoscopy training with u-tube and
facebook interfaces, numerous teachiing
videos, and step by step tesng and assess
ment tools
www.aabronchology.org American Associaon for Bronchology and I
ntervenonal Pulmonology (AABIP)
www.eabip.org European Associaon for Bronchology and
Intervenonal Pulmonology
W A B I P N E W S L E T T E R
Links
www.chestnet.org Intervenonal Chest/Diagnosc Procedures (IC/DP)
NetWork
www.thoracic.org American Thoracic Society
www.ctsnet.org The leading online resource of educaonal and
scienc research informaon for cardiothoracic
surgeons.
www.jrs.or.jp The Japanese Respirology Society
sites.google.com/site/asendoscopiarespiratoria/
Asociación Sudamericana de Endoscopía Respiratoria
P A G E 17