Volume 10
Issue 02
MAY 2022
Inside This Issue
Editorial, 2-4
Technology Corner, 5-6
Tips from the Experts, 7-9
Humanitarian News, 10-11
Best Image Contest, 12
WABIP News, 13
Research, 14-15
Links, 16
Patients with Complex Tracheal Disease Benefit from a
Multidisciplinary Airway Team
WABIP Newsletter
M A Y 2 0 2 2 V O L U M E 1 0 , I S S U E 2
EXECUTIVE BOARD
Hideo Saka, MD
Japan, Chair
Stefano Gasparini,
MD
Italy, Vice-Chair
Silvia Quadrelli, MD
Argenna, Immediate
Past-Chair
David Fielding MD
Australia, Treasurer
Naofumi Shinagawa,
MD
Japan,
Secretary General
Philippe Astoul, MD
France, President
WCBIP 2022
Menaldi Rasmin, MD
Indonesia, President
WCBIP 2024
STAFF
Michael Mendoza
General Manager
Judy McConnell
Administrator
Kazuhiro Yasufuku
Newsleer Editor-in-
chief
P A G E 2
Not uncommonly paents who present with dysp-
nea, wheezing, cough, or other respiratory symp-
toms are inially diagnosed as having asthma or
COPD, but ulmately found to have tracheal steno-
sis. This can be secondary to a number of condions
including but not limited to mechanical injury (e.g.
post intubaon, post tracheostomy) as well as con-
necve ssue disease, inhalaonal injury, radiaon,
and infecons (post tuberculosis, viral or tracheis
from Klebsiella rhinoscleromas or other organ-
isms). These tracheal abnormalies are found in
paents with varying comorbidies and many mes
present in the form of rm broc cicatrix, which
vary in degree of obstrucon, length, morphology,
and locaon, specically the distance from the cri-
coid carlage. As such, collaboraon within a mul-
disciplinary team of physicians with experse in
dierent techniques involving otolaryngologists,
thoracic surgeons, and intervenonal pul-
monologists ensures the most opmal management
for individual paents. In muldisciplinary airway
team meengs and clinics, the teams consider dier-
ent methods for management of tracheal diseases
including medical management alone, endoscopic
incisions and dilaon, stenng, or open surgical re-
secon (Figure 1).
Muldisciplinary management of complex airway
cases includes regular conferences to discuss these
paents and review their CT scans, laryngoscopy and
bronchoscopy videos. This is oen followed by
shared clinics for further evaluaon and joint proce-
dures in the operang room. Like other centers
across the world, at the University of Chicago we
have developed a formal Complex Airway Disease
Center, where paents are evaluated by our mul-
disciplinary team of physicians including interven-
onal pulmonology, ENT, and thoracic surgery. Cas-
es are reviewed at a monthly conference for shared deci-
sion-making and planning purposes. Notably, collaborave
management in the operang room is also frequently u-
lized for both airway assessment and therapeuc manage-
ment. In some cases, airway patency has to be restore
emergently via rigid bronchoscopy but an evaluaon by a
surgeon can be performed simultaneously, especially for
paents who are known to have complex stenosis and are
otherwise surgical candidates (Figure 2). Other mes, oto-
laryngology manages the subgloc laryngeal disease or
performed suspension laryngoscopy with jet venlaon,
while IP manages the tracheal component, especially in
inoperable paents with extensive, mulfocal disease or
those with acute necrozing tracheis casing airway com-
promise (Figure 3). Addionally, monthly meengs are held
with long-term acute care hospital partners to ensure op-
mal follow up for paents who may get transferred to such
a facility (especially post tracheostomy paents). We have
recently proposed an algorithm of muldisciplinary care
which is ulized by the members of our team (Figure 1) (1).
Another important service of the muldisciplinary complex
airway care team is to manage paents who develop short
or long-term tracheostomy-related adverse events. These
paents require careful management to ensure opmal
management of any tracheostomy-related issues including
but not limited to stomal strictures, subgloc stenosis,
stenosis/granulaon distal to the tracheostomy and trachea
-esophageal stulas. For inpaents, allied healthcare pro-
viders (nurses, physician assistants, or respiratory thera-
pists) with specialized training in tracheostomy manage-
ment should be involved for a consistent follow up and ear-
ly detecon of any tracheostomy-related issues and to as-
sure an opmal post procedure management (downsizing
the tracheostomy tube, capping trials, decannulaon). Ad-
dionally, speech and language pathologists are integral
members helping paents to resume speech funcon. Stud-
ies have described the approach to implementaon of tra-
Ajay Wagh
1
, Brandon Baird
2
, Maria Lucia Madariaga
3
, Elizabeth Blair
2
, Sepmiu Murgu
1
1
Secon of Pulmonary and Crical Care Medicine/Intervenonal Pulmonology, Department of Medicine, The University of
Chicago, Chicago, IL, USA
2
Secon of Otolaryngology, Department of Surgery, The University of Chicago, Chicago, IL, USA
3
Division of Thoracic Surgery, Department of Surgery, The University of Chicago, Chicago, IL, USA
Correspondence to: Ajay Wagh. Division of Intervenonal Pulmonology, The University of Chicago, 5841 S Maryland Ave,
Chicago, IL 60637, USA. Email: awagh@medicine.bsd.uchicago.edu.
W A B I P N E W S L E T T E R
P A G E 3
References:
1. Agrawal A et al. Respir Med. 2021;187:106582.
2. Crosbie R et al. J Laryngol Otol. 2014;128(2):171-3.
3. Norwood MG et al.. Postgrad Med J. 2004;80(946):478-80.
4. Meister KD et al. Otolaryngol Head Neck Surg. 2021;164(5):984-
1000.
5. Lamb CR et al. Chest. 2020 Oct;158(4):1499-1514.
cheostomy specialists and have demonstrated im-
proved outcomes with fewer complicaons and
crical incidents. Tracheostomy specialists can also
help to educate other sta members in tracheosto-
my management (2, 3). Since the beginning of
COVID-19 pandemic, there has been even more of
a need for careful tracheostomy management from
specialized care teams as described (4, 5).
Like in other areas of medicine, such as thoracic
oncology, engaging a muldisciplinary team of pro-
fessionals with dierent educaonal backgrounds
and skillsets can help oer opmal management
for complex airway paents. The group can also
collaborate and provide long term follow up care
required to ensure airway stability, evaluate for
recurrence in seng of malignancy resecon, and
to help migate any potenal complicaons.
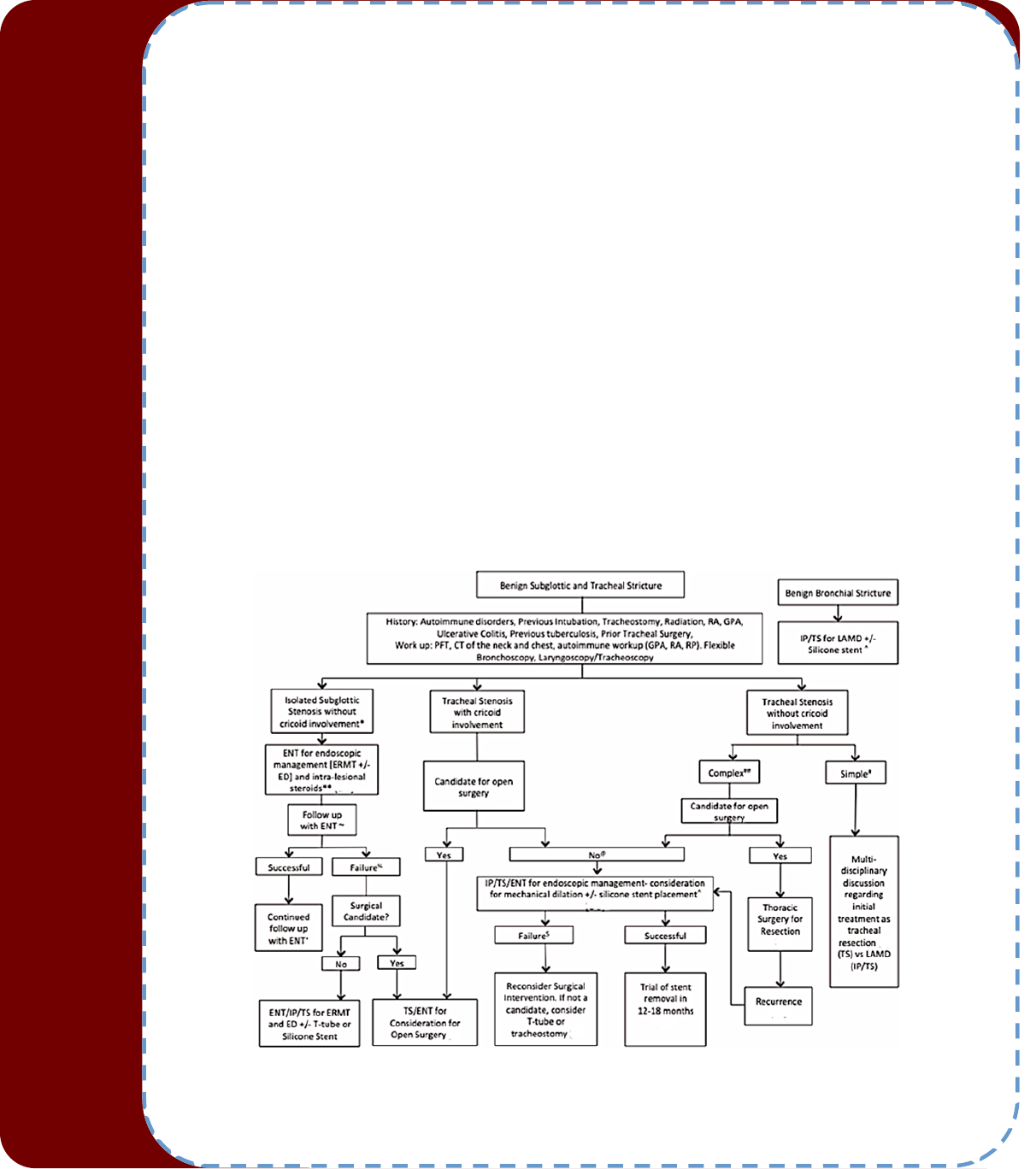
Figure 1. Muldisciplinary Benign tracheal stricture management per Agrawal et al (1). Used with permission from Elsevier.

W A B I P N E W S L E T T E R
P A G E 4
A Mul-disciplinary Management Algorithm in Paents with Benign Airway Strictures Mechanical Dilaon: LAMD (Laser As-
sisted Mechanical Dilaon) or Cold Knife Assisted Mechanical Dilaon. ERM'T: Endoscopic resecon (+/- Wedge Approach)
with adjuvant medical therapy (PPI, ICS and TMP/SMX). ED: Endoscopic Dilaon, ENT: Ear, Nose & Throat Surgery, IP: Inter-
venonal Pulmonology, TS: Thoracic Surgery. *This algorithm applies only to idiopathic subgloc stenosis (iSGS). For paents
with connecve ssue disorders, rst treatment opon will be endoscopic management due to high recurrence rate post-
surgical resecon. ** Endoscopic management depending on severity of symptoms. Paent will undergo radial incision with
or without mechanical dilaon. ~ Outpaent follow up with ENT including outpaent laryngoscopy and in-oce injecon of
intralesional steroids. % Failure dened as paents requiring more than 3 intervenons over 2-3 years with symptomac re-
currence and >50% stenoc index, despite oce-based intralesional corcosteroid injecon. + Consider use of oce based
intralesional steroid injecon to maintain patency and reduce me to re-intervenon. *# Complex: Longer> 1 cm, with or
without chondris. # Simple: Less than 1 cm in size, without chondris. @ Factors aecng surgical candidacy include mulple
comorbidies, prolonged steroid use, stricture locaon, or long vercal extent (>4-6 cm). § Failure dened as repeated proce-
dures including recurrent stent migraon, followed by symptomac recurrence of stenosis. All paents with airway stent will
follow the stent protocol dened below. Stent Follow-up Protocol: Flexible Bronchoscopy with moderate sedaon 4-6 weeks
post stent placement. Follow up bronchoscopy every 2-3 months or based on clinical symptoms. 0.9% Normal saline nebulizer
5-10 ml TID. Stent card & Stent educaon.
Figure 2. Severe PITS in a paent with respiratory distress seen
during rigid bronchoscopy (top le). Laser assisted mechanical
dilaon restored airway patency (top right). At the me of recur-
rence, the paent underwent surgical resecon. The le boom
le panel shows the marked proximal and distal aspects of the
stenosis. The excised tracheal stenosis segment of ~ 3 cm is seen
on the boom right panel.
Figure 3. Top panel. Severe tracheal stenosis developed distal to the p of a tracheostomy tube (picture A taken aer the
tracheostomy tube was removed). Post dilaon, a mucosal tear caused bleeding from the posterior tracheal wall which was
successfully coagulated using electrosurgery via tracheal stoma by the ENT surgeon (B and C). Then a T tube was inserted and
via rigid bronchoscopy using rigid forceps, the bronchoscopist assist in opening up the infra-stomal arm of the T tube (D).
Boom panel: E. severe symptomac pseudomembranous tracheal stenosis immediately post extubaon seen during exible
bronchoscopy. F. Suspension micro-laryngoscopy was performed by the ENT surgeon with Jet venlaon. G. Rigid broncho-
scopic debridement of the pseudo-membranes is performed. H. Then the stricture is dilated and airway patency is restored.
W A B I P N E W S L E T T E R
P A G E 5
Technology Corner
3D Prinng for Surgical Planning for Subgloc Airway Stenosis
Introducon
The surgical treatment of subgloc cicatricial stenosis remains one of the most challenging elds in airway surgery. In addi-
on to the esmated resecon length, the proximity of the stenosis to the vocal folds is the main characterisc dictang
the appropriate surgical technique. Not only a complete resecon of the cicatricial ssue, but also preservaon and resto-
raon of the funconal capacies of the larynx should be achieved. In general, the pre-operave work-up in paents with
airway stenosis should at least consist of a computed tomography (CT) and bronchoscopy. However, even for experienced
surgeons the pre-operave judgement of the exact extent of the stenosis and the required surgical repair remains demand-
ing, especially in subgloc pathologies.
Background
Addive manufacturing and three-dimensional (3D) prinng is nowadays broadly available. Consequently, a growing num-
ber of possible medical applicaons has been described. Especially in the diagnosis and treatment of airway pathologies, a
variety of possible applicaons were described by various instuons world-wide (1-4). Beyond manufacturing customized,
paent-specic implants such as airway prosthesis (4), the transion of two-dimensional CT images into 3D-printed, hap-
cally percepble models changed the possibilies of teaching and planning complex surgical procedures (5). For instance,
3D-printed models of centrally located lung cancer can be used to teach surgical residents the principles of bronchial sleeve
resecons (6). Using materials with similar rigidity and elascity as the human airways, bronchial sleeve resecons were
even simulated in a simplied, but anatomically correct way during dry lab trainings. Similarly, 3D printed models can also
be used to plan complex resecon at the laryngotracheal juncon.
Dependent on the extent of subgloc stenosis in relaon to the anatomical structures, various surgical techniques have
been described. Cricotracheal resecon including a paral resecon of the cricoid arch and the rst tracheal rings is consid-
ered the basic technique to address a stenosis, which is limited to the anterior poron of the cricoid. A dorsal mucosectomy
at the cricoid plate has to be added to the procedure, as soon as the scaricaon of the mucosa or submucosa is present at
the dorsolateral poron of the cricoid. This involvement is rather typical in paents suering from an idiopathic subgloc
stenosis. The most complex type of subgloc stenosis reaches the vocal fold and is therefore described as gloo-subgloc
stenosis. If a complete resecon by means of a cricotracheal resecon with a very extended dorsal mucosectomy is not
resulng in a sucient subgloc lumen, the larynx has to be enlarged by the interposion of carlage anteriorly and/or
posteriorly.(7) Although the ulmate decision which of these techniques has to be made during the surgical procedure,
experienced airway surgeons will be able to predict the necessary surgical technique with a very high accuracy. However,
students, residents and surgeons not experienced in airway surgery usually exhibit dicules in merging bronchoscopic
ndings with the corresponding CT images. Subsequently, the incorrect classicaon of the airway stenosis negavely
aects planning the appropriate surgical procedure.
Thomas Schweiger, MD, PhD,
1
Kazuhiro Yasufuku, MD, PhD,
2
Konrad Hoetzenecker, MD, PhD
1
1 Department of Thoracic Surgery, Medical University of
Vienna, Austria.
2 Division of Thoracic Surgery, Toronto General Hospital,
University Health Network, Toronto, Ontario, Canada
W A B I P N E W S L E T T E R
P A G E 6
Clinical Applicaon
We could previously demonstrate the value of 3D-printed models over convenonal CT images or bronchoscopy in paents
with subgloc stenosis. (8) In this work, the study parcipants were divided into subgroups dependent on the level of ex-
perience in airway surgery (residents vs. fellows or non-airway surgeons vs. dedicated airway surgeons). Parcipants were
provided with bronchoscopy videos, convenonal CT scans or 3D-models of 19 paents with subgloc stenosis and asked
to classify the stenosis and to choose the appropriate surgical technique for resecon. Residents and fellows/non-airway
surgeons beneted most from the 3D models which signicantly improved their diagnosc accuracy. Interesngly, the
group of experienced airway surgeons achieved almost a similar high accuracy by sole evaluaon of bronchoscopy videos.
Two-dimensional axial CT images were of least value throughout all study groups. This study illustrated the potenal bene-
ts of 3D models when treang paents with subgloc stenosis. Moreover, these models might be of value in paent edu-
caon and when obtaining informed consent for laryngotracheal resecons. 3D models could be used to illustrate specic
surgical procedures and possible funconal implicaons aer surgery to the paent. However, there also several issues
liming the clinical applicaons of these 3D printed models. First, processing of the raw imaging data to delineate the ste-
nosis from the individual anatomical structures and mul-color prinng requires a degree of knowledge and resources,
which are not available at every instuon. Moreover, manufacturing a 3D model for each individual paent referred for
surgery would most likely exceed these capacies even if present and established. The me needed from imaging acquisi-
on to the producon of a model is rather weeks than days, dependent on the available infrastructure and personnel. Last,
the diagnosc benet decreases with growing experience of the surgeon. Thus, prinng a 3D model of each paent receiv-
ing laryngotracheal surgery might not be feasible, and also not necessary.
In summary, a set of 3D models of typical and also exceponal cases can contribute to a deeper understanding of complex
airway stenoses. 3D models should be considered an addional way to visualize a surgical problem in a comprehensive
manner.
Conclusions
3D printed airway models are a tool which can increase the diagnosc accuracy of subgloc stenosis and improve surgical
planning of a resecon. The broad availability of 3D prinng and the relavely easy access will foster the use of these mod-
els in training and in clinical pracce.
References:
1. Tsai A et al. JTCVS Tech 2021;ahead of print.
2. Les AS et al. Laryngoscope 2019;129:1763-71.
3. Kamran A et al. JTCVS Tech 2021;8:160-9.
4. Schweiger T et al. J Thorac Cardiovasc Surg 2018;156:2019-21.
5. Leung G et al. S Int J Pediatr Otorhinolaryngol 2022;155:111083.
6. Hashimoto K et al. JTCVS Techniques 2022;online, ahead of print.
7. Schweiger T et al. J Thorac Cardiovasc Surg 2022;163:313-22 e3.
8. Hoetzenecker K et al. Ann Thorac Surg 2019;107:1860-5.

Tips from the Experts
P A G E 7 V O L U M E 1 0 , I S S U E 2
Introducon:
Tracheal or laryngotracheal stenosis may result from a broad spectrum of underlying eologies including gastroesophageal reux disease,
systemic disorders such as scleroderma or sarcoid, infecon, malignancy, or radiaon injury. At mes, the cause of the stenosis cannot be
specied, and is termed idiopathic. However, internal trauma due to endotracheal intubaon or tracheostomy is the most common cause of
acquired stenosis.
1
The dramac rise in mechanical venlaon due to the COVID-19 pandemic further solidies this as a causave frontrun-
ner.
2
While endoscopic intervenons are oen rst-line therapy for symptom palliaon, recurrence is common. Surgical resecon and air-
way reconstrucon oers denive treatment with high rates of success.
3,4
Paent Evaluaon and Indicaons:
Paents with acquired tracheal stenosis typically present with a history of dyspnea exacerbated by exeron which may progress to wheez-
ing or stridor in the seng of advanced disease. Symptoms severe enough to rise to medical aenon typically occur when stenosis has
reached at least 50% of the airway diameter and inial misdiagnosis with more common respiratory ailments is common.
5,6
Workup includes
pulmonary funcon tests, serologic evaluaon for anneutrophil cytoplasmic anbodies, and computerized tomography (CT) of the neck
and chest. Dynamic CT may facilitate idencaon of tracheomalacia which may accompany tracheal stenosis in select paents. Grading
systems include the Myer-Coon system which is based on stenoc severity and the McCarey system which categorizes based on locaon
and length of stenosis.
7,8
Bronchoscopy is the gold standard diagnosc technique and remains essenal to evaluang surgical candidacy. While rigid bronchoscopy
has been promoted in paents with more severe symptoms,
1
we have found exible bronchoscopy to be sucient in the majority of pa-
ents. We typically perform this with the paent under general anesthesia but without paralycs in order to evaluate vocal cord funcon
and the degree of airway collapse due to associated tracheomalacia. The procedure is performed with a laryngeal mask airway in place and
temporary removal of the tracheostomy tube, if present, to allow thorough evaluaon of the airway. Key components of the exam include
assessment of: (1) type of lesion, (2) locaon of stenosis including involvement of the cricoid carlage, (3) length of stenosis, (4) involvement
of other structures, notably the proximal larynx, (5) gloc aperture, (6) recurrent laryngeal nerve funcon, and (7) length of normal trachea.
In the seng of subgloc stenosis, assessment of the subgloc aperture is crical to successful surgical resecon; this region must be of
sucient diameter and free of inammaon or other mucosal abnormality. (Figure 1)
There is no age threshold that precludes a paent from surgical consideraon and the procedure is generally well tolerated even in older,
frail paents. However, there are several pre-exisng condions that warrant careful consideraon during preoperave evaluaon. While
paents with borderline pulmonary funcon oen tolerate tracheal resecon, surgery should be avoided in those who are likely to require
postoperave mechanical venlatory support, or paents with condions that put them at high risk of requiring intubaon postoperavely,
such as individuals with poorly controlled myasthenia gravis prone to respiratory decompensaon. In addion, paents with pre-exisng
neurologic dysfuncon pose a parcular challenge to successful surgery, as paent cooperaon with airway clearance and tolerance of the
guardian stch to avoid excessive head movement postoperavely is crical. Similarly, any suggeson of aspiraon needs to be thoroughly
invesgated preoperavely. These paents may require tracheostomy permanently or unl neurologic funcon improves. Finally, modia-
ble risk factors including obesity and steroid use should be reced prior to surgery.
Open Surgical Approach to Tracheal Stenosis
John D Mitchell, MD
Davis Endowed Chair in Thoracic Surgery
Professor and Chief, General Thoracic
Surgery
University of Colorado
Lauren Taylor, MD
Chief Resident, Cardiothoracic
Surgery
Tips from the Experts
P A G E 8 V O L U M E 1 0 , I S S U E 2
Procedural Consideraons:
There is rarely an indicaon for emergent tracheal resecon; surgery in this seng may be fraught with complicaons. Paents in extremis
are oen beer served with tracheostomy or endoscopic intervenon such as dilaon to secure the airway with plans for formal surgical re-
secon and reconstrucon aer their condion has temporized. Similarly, it is prudent to delay resecon in the seng of acve infecon
near the operave eld as well as excessive local inammaon due to recent tracheostomy or dilaon.
A key to successful tracheal resecon and primary anastomosis is determinaon of how much trachea may be removed safely. Over the
years, invesgaons performed in animals and human cadavers have measured anastomoc tension with various lengths of resecon in an
aempt to answer this queson.
9-12
Unfortunately at present no reliable means of intraoperave measurement of anastomoc tension exists
and this technique is not rounely used in pracce. While precise limits of tracheal resecon remain elusive, about 50% of the adult trachea
may be safely removed in most cases. It is generally accepted that permissible lengths vary based on paent age, body habitus, and history of
prior neck or chest surgery that may limit tracheal mobility due to scarring. For a stenosis of the proximal airway, neck exion as well as surgi-
cal release maneuvers such as mobilizaon of the pre-tracheal plane or suprahyoid laryngeal release have been shown to decrease anasto-
moc tension and allow surgeons to push the boundaries of resecon; for distal airway stenosis, a hilar release can aord similar advantages.
Resecon of subgloc stenosis is typically performed through a collar incision, with excision of the stoma site if a tracheostomy was present.
Addional upper neck incision, sternotomy, or thoracotomy may be required in some instances depending on locaon of the tracheal lesion
and need for release maneuvers. Neck extension is achieved through careful paent posioning with a pillow between the scapulae and is
crical to ensure adequate exposure of the operave eld. In addion, bronchoscopy may be used intraoperavely to localize the lesion at
the me of tracheal transecon.
Subgloc stenosis poses parcular surgical challenges due to the relavely narrow caliber of the laryngotracheal region and parcular care
must be taken to preserve the vocal cords when cricoid resecon is necessary. The anastomosis is performed in an end-to-end fashion using
interrupted absorbable sutures. We commonly use a strap muscle to buress the anastomosis and prevent stula development. At the me
of primary anastomosis, the paent’s neck is moved to a exed posion to minimize tension. We typically do not place T-tubes but favor
placement of a guardian stch prior to extubaon to limit neck mobility during the rst week aer surgery.
An experienced anesthesia team is essenal and constant communicaon between surgeon and anesthesiologist is needed to ensure surgical
success. A variety of airway management strategies during tracheal resecon have been described. While surgical cross-eld intubaon and
jet venlaon are the most well-established, newer techniques have been proposed including use of supragloc airways, regional anesthe-
sia, and extracorporeal support.
13,14
We favor endotracheal intubaon aer inducon of general anesthesia with a small caliber endotracheal
tube as needed to accommodate the degree of stenosis. Aer tracheal transecon, the surgeon places an armored endotracheal tube distally
in the airway and cross-eld venlaon is used unl the anastomosis is complete.
Postoperave Care and Surveillance:
The majority of paents are extubated in the operang room at the conclusion of surgery. If ongoing mechanical venlaon is necessary, it is
essenal to ensure that the cu of the endotracheal tube is posioned distal to the anastomosis with minimal inaon. Decadron may be
indicated for some paents if signicant laryngeal edema is present. All of our paents are monitored in the intensive care unit and kept nil
per os for the rst 24-48 hours postoperavely unl formal swallow evaluaon is complete. We keep the guardian stch in place unl post-
operave day 7 at which me bronchoscopy is performed. If the anastomosis is healing appropriately, the stch is removed along with surgi-
cal drains and the paent is discharged home.
We rounely follow paents with serial bronchoscopic evaluaons aer hospital discharge. (Figure 2) This facilitates early detecon of anas-
tomoc complicaons and allows for intervenons such as debridement of granulaon ssue or dilaon of anastomoc strictures. In the
seng of tracheal resecon for tumor, bronchoscopy also serves the added role as surveillance of cancer recurrence.
Surgical Complicaons and Outcomes:
Complicaons of tracheal resecon and reconstrucon have been minimized with advances in surgical technique. However, a variety of anas-
tomoc and other complicaons may sll arise. Formaon of granulaon ssue at the anastomosis is one of the more common complicaons
(although less frequent with the use of absorbable suture) and may be addressed by vigilant bronchoscopic follow-up postoperavely. Excess
anastomoc tension or impaired tracheal blood supply due to over-dissecon may lead to necrosis, separaon or stricture that may be rec-
ed with endoscopic techniques or in some instances require re-resecon. Hemorrhage due to innominate artery erosion may occur if care is
not taken to ensure that the artery does not rest in direct contact with the anastomoc sutures. Similarly, vocal cord dysfuncon and subse-
quent aspiraon may result from an error in surgical technique and failure to protect the nerves during tracheal dissecon. A rare but debili-
tang complicaon to consider during paent posioning is quadriplegia due to extreme cervical exion or extension.
Despite known complicaons, contemporary literature reports improved surgical outcomes. A recent retrospecve analysis of 228 consecu-
ve laryngotracheal resecons performed over the last decade demonstrates 0% perioperave mortality rate. The overall complicaon rate
was 9.6%; 7.8% are aributed to airway complicaons with the most common being restenosis. At a mean follow up of 65.5 months, deni-
ve treatment success was achieved in 98.7% of paents.
3
Similar success was reported by Wang and colleagues in 2015 with 96% of paents
who underwent surgical resecon for idiopathic subgloc stenosis achieving good to excellent postoperave results.
15
Findings reported by
Tips from the Experts
P A G E 9 V O L U M E 1 0 , I S S U E 2
D’Andrilli et al. echo these results with denive good or excellent results in 94.5% of their cohort and a complicaon rate of 9.2%.
4
Conclusions:
Surgical resecon and reconstrucon oers denive treatment of tracheal stenosis with recent literature demonstrang encouraging trends
in improved postoperave outcomes. Surgical treatment of this disease is likely to play an increasingly prominent role due to the prevalence
of mechanical venlaon aributed to the COVID-19 pandemic. Adherence to meculous surgical techniques and the parcipaon of experi-
enced teams in high-volume centers is important to ensure surgical success, parcularly in the seng of subgloc stenosis.
References:
1. Aravena C et al. J Thorac Dis. 2020;12(3):1100-1111. doi:10.21037/jtd.2019.11.43
2. Piazza C et al. Eur Arch Otorhinolaryngol. 2021;278(1):1-7. doi:10.1007/s00405-020-06112-6
3. Maurizi G et al. J Thorac Cardiovasc Surg. 2021 Mar;161(3):845-852. doi: 10.1016/j.jtcvs.2020.12.023. Epub 2020 Dec 14. PMID: 33451851.
4. D'Andrilli A et al. Eur J Cardiothorac Surg. 2016 Jul;50(1):105-9. doi: 10.1093/ejcts/ezv471. Epub 2016 Jan 19. PMID: 26792926
5. Maldonado F et al. Orphan Tracheopathies. In: Con V, Cordier JF, Richeldi L, editors. Orphan Lung Diseases. London: Springer London, 73-89.
6. Costanno CL et al. J Thorac Dis 2016;8:S204-9.
7. McCarey TV. Laryngoscope 1992;102:1335-40. 10.1288/00005537-199212000-00004
8. Myer CM et al. Ann Otol Rhinol Laryngol 1994;103:319-23. 10.1177/000348949410300410
9. Cantrell JR et al. J Thorac Cardiovasc Surg 1961;42:589–98.
10. Kotake Y et al. J Thorac Cardiovasc Surg 1976;71:600–4.
11. Michelson E et al. J Thorac Cardiovasc Surg 1961;41:748–59.
12. Grillo HC et al. J Thorac Cardiovasc Surg 1964;48:741–9.
13. Schieren M et al. J Cardiothorac Vasc Anesth. 2017 Aug;31(4):1351-1358. doi: 10.1053/j.jvca.2017.03.020. Epub 2017 Mar 24. PMID: 28800992.
14. Schieren M et al. Anesth Analg. 2018 Apr;126(4):1257-1261. doi: 10.1213/ANE.0000000000002753. PMID: 29293182.
15. Wang H et al. Ann Thorac Surg.2015;100:1804-11.
Figure 1: Preoperave exible bronchoscopy demonstrates signi-
cant subgloc stenosis. This paent was deemed to be a suitable
operave candidate and underwent laryngotracheal resecon.
Figure 2: Postoperave surveillance bronchoscopy in the paent with
subgloc stenosis who underwent laryngotracheal resecon demon-
strates that the anastomosis is healing well without evidence of stric-
ture.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 10
PARAGUAY PROJECT
In November 2021 the World Bronchology Foundaon (WBF) received, from Paraguay, a request for help to treat paents
with post-intubaon tracheal stenosis due to COVID. Concretely, Dr Domingo Regalado Pérez asked the Foundaon for a
rigid bronchoscope and for providing training to deal with this unforeseen diculty of the COVID pandemic. Dr Domingo
Regalado Pérez is the head of the Pneumology Service of the General Luque Hospital, which belongs to the Ministry of Public
Health in Paraguay, and is also a member of the WBF Board. The aim of the Project was to bring a rigid bronchoscope with
opcs, light source, camera and forceps and to conduct a course-workshop on the use of the rigid bronchoscope and thorac-
ic ultrasound. For this project, support and funding was sought from the Asociación Española de Endoscopia Respiratoria y
Neumología Intervencionista (AEER), the Sociedad Española de Neumología y Cirugía Torácica (SEPAR) and help from the
commercial companies Ibersurgical and Suministros Hospitalarios. For this project, the AEER, and SEPAR gave nancial sup-
port, while the companies Ibersurgical and Suministros Hospitaraios gave material”. The culminaon of the project consisted
in a week-long trip to Paraguay which took place the last week of March 2022 where three professionals were awarded to
take part in the trip, Dr. Javier Flandes and Dr. Enrique Cases by AEER and the nurse Susana Alvarez by SEPAR. Prior to the
trip, all the expected material was obtained, as well as various prostheses and dierent endoscopic material, so that the
budget reached for this project was around 25,000 €.
Once in Paraguay, the rst day of the course-workshop was held at the Hospital Central del IPS-Asunción, where a series of
lectures on rigid bronchoscopy and thoracic ultrasound were given. It is worth menoning the presentaon on broncho-
scope reprocessing given by nurse Susana Alvarez, as the lecture aroused a lot of interest among the aending doctors. In
addion, during the second they of the course, nurse Susana had the opportunity to collaborate with the nurses working at
above menoned hospital, as well as with nurses working in other hospitals from Auncion and Luque. Not only she was able
to collaborate but also to conduct presentaons and workshops on reprocessing, sedaon and the handling of endoscopic
samples.
The following days of the Course-Workshop were held at the Hospital General of Luque. Luque is a city of Paraguay located
in the Central Department near to Asunción which is the current capita of Paraguay. In this hospital were addressed topics
related to the rigid bronchoscopy and thoracic ultrasound as well as other issues such as the diagnosc and therapeuc pos-
sibilies of the cryoprobe, thermoplasty, the endoscopic diagnosc possibilies of the pulmonary nodule or pleural patholo-
gy were developed. In this hospital, we had the possibility to parcipate in the treatment of two paents suering from tra-
cheal stenosis. The paents were treated with the new rigid bronchoscope and were placed a Dumon prosthesis and a
Leufen prosthesis donated by Suministros Hospitalarios. Thanks to the opcal and camera equipment donated by Ibersurgi-
cal, the two intervenons were visualised by the young pneumologists. Thoracic ultrasound scans were also performed in
dierent departments of the hospital to familiarise the pneumologists with the dierent pathologies and some specic diag-
noses were made, such as a diaphragmac paralysis in a venlated paent who was dicult to wean.
The course was aended by around twenty-ve young pulmonologists from dierent cies of Paraguay who showed their
enthusiasm for intervenonal pneumology and their eagerness for training in this eld. We would like to thank the Sociedad
Paraguaya de Neumología and its president Dr. José Oviedo for their warm welcome and for the logiscal and technical sup-
port we were given, without which this project would not have been possible. We would also like to thank the pneumolo-
gists Dr Domingo Pérez, soul of the Project in Paraguay, Dr Gilberto Chaparro whose experience in intervenonal bronchos-
copy we consider fundamental for the further development of this Project, the young pneumologists who parcipated t in
the course and the members of the Pneumology Service of the General Hospital of Luque in whose hands lies the future of
intervenonal pneumology in Paraguay, Dr Diego Medina, Dr Avid Aluan, Dr Silvio Benitez, Dr Liza Davalos, Dr Sergio Cárde-
nas, Dr Diego Aguayo and Dr Carlos Pallarolas.
In addion to this Project in Paraguay and the previous Projects developed with AEER and SEPAR Solidaria in Panama, El Sal-
vador and Honduras in 2018, the WBF parcipated in the SEPAR Solidarity Project held in the Sahrawi Refugee Camps in Al-
giers. In this project, a GeneXpert was brought for the diagnosis of tuberculosis and which has been fundamental for the

Humanitarian News
W A B I P N E W S L E T T E R P A G E 11
diagnosis of COVID in this Camp. There is a project underway to bring a bronchoscope to the camp and to provide training to
a digesve endoscopist to work in the refugee camp, because the camp does not have a pulmonologist and there are nearly
200,000 people living there with limited means and depending on external aid.
Best Image Contest 2022 (2 of 3)
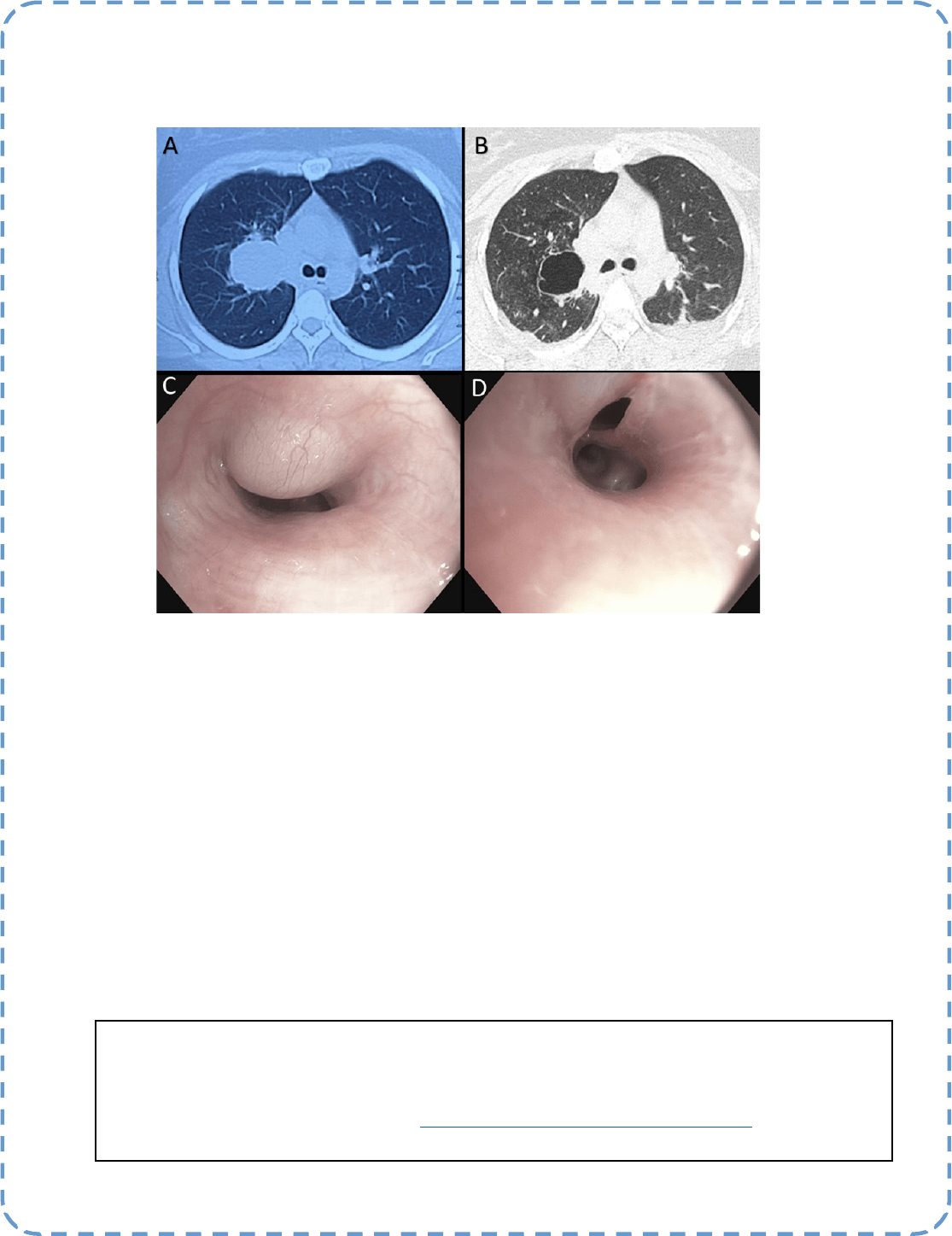
Descripon:
Spontanous rupture of Bronchogenic Cyst
A- Axial CT view of the bronchogenic cyst before rupture
B- Axial CT view of the bronchogenic cyst aer rupture
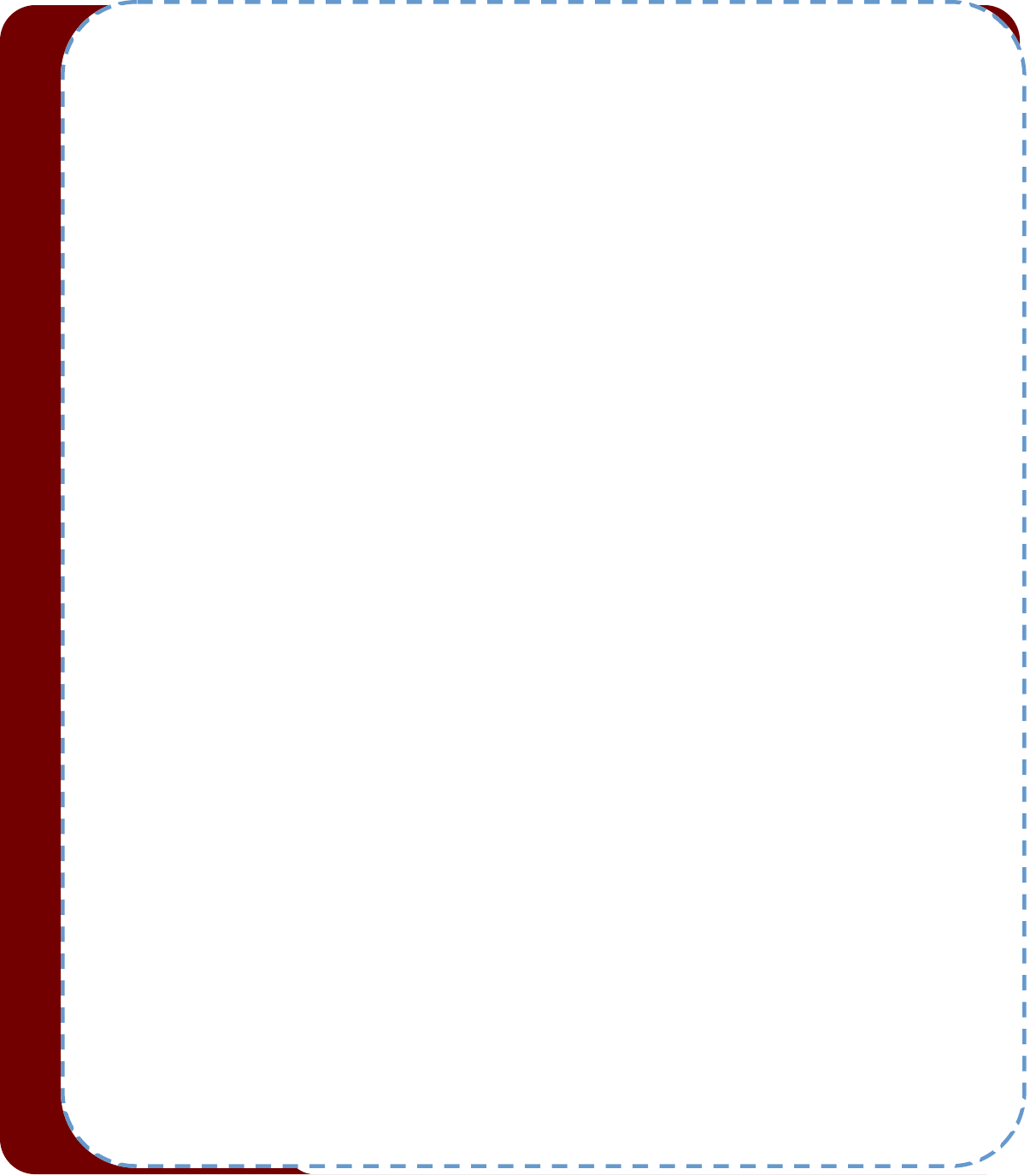
C- Bronchoscopy view of intact bronchogenic cyst in the right upper lobe
D- Bronchoscopic view of ruptured bronchogenic cyst causing breach on the bronchial wall
Submier:
Dr. Roshan Kumar
Best Image Contest
P A G E 12
This image is the 1 of 3 selected among 100+ submissions to our Best Image Contest held in late 2021. Please
stay tuned to the next Image Contest opening later this year. Find the above image and more at the WABIP
Academy Image Library at hps://www.WABIPacademy.com/imagelibrary
P A G E 13
WABIP News
WCBIP 2022 Registraon Discounts Ending Soon
Take advantage of registraon discounts of up to 33% unl July 15, 2022 for WCBIP Marseille
2022. If you register for "remote access" (virtual) rst, you can upgrade to on-site access at any
me, even at the venue. In which case, the price dierence will be invoiced.
REGISTER NOW at hps://www.wcbip.org/general#fees
WABIP Vice Chair Nominaons
Nominaons for the next WABIP Vice-chair are sll open unl July
1, 2022. If you would like to consider a colleague for the chance to
be the next Vice-chair, you may nominate by downloading and
compleng the following form @ hps://cdn.wabip.com/
downloads/vice-chair/WABIP-Vice-Chair-Nominaon-Form-
2022.pdf
WCBIP 2026 Bids
As the above, the deadline for WCBIP bids applicaons is July 1,
2022. We cordially invite you to submit a bid for organizing our
biennial congress which shall take place 4 years from now. Down-
load and complete the following form to begin @ hps://
www.wabip.com/news/544-wcbip2026bids2
WABIP Awards
Celebrate and give recognion to your outstanding colleague in the
IP community by nominang him or her for a WABIP Award. Nomi-
naons for the Killian Medal, the Dumon Award and the Lifeme
Achievement Award are due by July 1, 2022. You may nominate
yourself for the Becker Award upon subming an abstract for
WCBIP 2022. More details at hps://www.wabip.com/awards
WABIP Board of Regents Meeng in Marseille
We are pleased to announce that the next BOR meeng will be held in Marseille on-site this October 6, 2022 at
1:00 pm CEST. For those who cannot aend on site, Regents may join via Zoom. This meeng will include elecons
for next WABIP Vice-chair and vong for WCBIP 2026 host site, as described above. General members: please be
sure to contact your society representave (Regent) so that he/she may represent your vote.
The Mantra of Medicine
Muldisciplinary Approach and Personalized Therapy
Idiopathic subgloc stenosis (ISGS) is a rare (1:400,000), recurrent, broinammatory disease that results in debilitang and life-threatening air-
way obstrucon. While ISGS is a rare condion, it is well-known to intervenonal pulmonologists, laryngologists, and thoracic surgeons.
Causes of ISGS include congenital, trauma such as intubaon or tracheostomy, inammatory condions, and idiopathic diseases. This disease can
lead to debilitang symptoms such as dyspnea, cough, hoarseness, stridor, and sleep apnea. Oen the management opons are limited, invasive,
or subopmal, with recurrences requiring repeated intervenons. In many cases, quality of life is severely aected. Unfortunately, due to the
young age of paents in most of these cases, the impact of this disease is felt even more.
As intervenonal pulmonologists, we oen ulize rigid bronchoscopic dilaons, endobronchial ablave therapies, injecons of anbroc agents
such as steroid and mitomycin, and airway stenng. Our colleagues in ENT usually perform balloon dilaons and CO2 laser ablaon with or without
anbroc injecon, while thoracic surgeons perform cricotracheal resecon (CTR) and end to end anastomosis of the trachea in select cases when
feasible. The treatment approaches are oen instuon and provider-dependent. As we all have been taught in our training, rare and complex
diseases like ISGS should have a muldisciplinary approach to provide personalized therapy at expert centers. This oers the best chance to give
paents a long-term and denive treatment.
A large study (1) recently tried to answer the quintessenal queson of the best treatment strategy for ISGS. The study prospecvely compared the
outcomes of the three most common approaches for managing ISGS. It recruited ISGS paents with or without previous treatment from mulple
centers across the United States in a prospecve manner. The study's primary endpoint was the me between the inial and second procedures.
Secondary endpoints of the study included quality of life, voice handicap, eang assessment, funconal health, and postoperave complicaons.
Eight hundred and ten paents were enrolled in the study. Inial surgical procedures were endobronchial dilaon (n = 603; 74.4%), endobronchial
Editor-in-Chief: Dr. Kazuhiro Yasufuku
Research
Primary Business Address:
Kazuhiro Yasufuku, Editor-in-Chief WABIP
Newsleer
c/o Judy McConnell
200 Elizabeth St, 9N-957
Toronto, ON M5G 2C4 Canada
E-mail: newsleer@wabip.com
P A G E 14
Associate editor:
Dr. Ali Musani
Associate editor:
Dr. Sepmiu Murgu
Ali I. Musani MD, FCCP
University of Colorado School of Medicine,
Denver
resecon and medical therapy (n = 121; 14.9%), and surgical therapy with CTR (n = 86; 10.6%). Overall, 22.8% of paents had a recurrent
surgical procedure during the 3-year study. However, the recurrence rates diered in three treatment groups, CTR, 1.2%; endobronchial
with medical therapy, 12.4%; and endobronchial dilaon, 28.0%. Among successfully treated paents without recurrence, those treated with
CTR had the best quality of life, the worst voice symptoms, and the most signicant perioperave risk. The most used therapeuc approach,
endoscopic dilaon, was associated with a higher recurrence rate than other procedures. In contrast, endoscopic resecon with medical
therapy (treatment of choice by the intervenonal pulmonologists) was associated with beer disease control than endoscopic dilaon and
had a minimal associaon with vocal funcon.
This study substanates the algorithmic approach of ISGS in a muldisciplinary fashion. In our pracce, every ISGS paent is referred to tho-
racic surgery for CTR if feasible. Unfortunately, most paents do not qualify for CTR due to confounders, including stenosis too close to the
vocal cords, long previous surgeries, and anatomical and medical issues. Our second line of treatment for ISGS is an intervenonal pulmonol-
ogy comprehensive approach with endotracheal resecon/debulking and dilaon with rigid bronchoscopy and endotracheal steroid injec-
ons, with or without stent and ablave therapies such as laser or cautery. Stents and ablave therapies are uncommonly used nowadays.
Our other adjuvant strategies include robust medical and behavioral control of gastroesophageal reux disease, management of hiatal her-
nia if contribung to reux, aggressive treatment of obesity, and workup and treatment of autoimmune diseases.
The answer to the queson as to the best approach for these paents remains, "it depends"! It depends on the locaon of the stenosis,
comorbidies, other confounding issues as menoned above, and perhaps most importantly, the experse of the treang instuons and
physicians. Hence, the mantra of "muldisciplinary approach to oer personalized therapy." Furthermore, as menoned earlier, the key is to
refer these paents to the expert centers once the diagnosis is established and the inial treatment is provided to prevent acute respiratory
compromise. This strategy has been proven to oer paents the best chance of meaningful recovery and the best quality of life.
Reference:
1. Gelbard et al. JAMA Otolaryngol Head Neck Surg. 2020 Jan 1;146(1):20-29.
Research
P A G E 15
P A G E
16
WABIP ACADEMY- WEBCASTS
The WABIP has started a new educaon project recently: THE WABIP ACADEMY. The WABIP Academy will pro-
vide free online webcasts with new and hot topics that will interest pulmonologists and intervenonalists.
Current webcast topic: Tissue acquision for biomarker directed therapy of NSCLC
You can reach these webcasts by using this link: hp://www.wabipacademy.com/webcast/
www.bronchology.com Home of the Journal of Bronchology
www.bronchoscopy.org Internaonal educaonal website for
bronchoscopy training with u-tube and
facebook interfaces, numerous teachiing
videos, and step by step tesng and assess
ment tools
www.aabronchology.org American Associaon for Bronchology and I
ntervenonal Pulmonology (AABIP)
www.eabip.org European Associaon for Bronchology and
Intervenonal Pulmonology
W A B I P N E W S L E T T E R
Links
www.chestnet.org Intervenonal Chest/Diagnosc Procedures (IC/DP)
NetWork
www.thoracic.org American Thoracic Society
www.ctsnet.org The leading online resource of educaonal and
scienc research informaon for cardiothoracic
surgeons.
www.jrs.or.jp The Japanese Respirology Society
sites.google.com/site/asendoscopiarespiratoria/
Asociación Sudamericana de Endoscopía Respiratoria
P A G E 16