Volume 10
Issue 01
January 2022
Inside This Issue
Editorial, 2-3
Technology Corner, 4-6
Tips from the Experts, 7-9
Humanitarian News, 10-16
Best Image Contest, 17
WABIP News, 18
Research, 19-20
Links, 21
Ali Musani MD, FCCP
University of Colorado School of Medicine
Artificial Intelligence and Interventional Pulmonology
Are we “stepping in GOD’s shoes”?
WABIP Newsletter
J A N U A R Y 2 0 2 2 V O L U M E 1 0 , I S S U E 1
EXECUTIVE BOARD
Hideo Saka, MD
Japan, Chair
Stefano Gasparini,
MD
Italy, Vice-Chair
Silvia Quadrelli, MD
Argenna, Immediate
Past-Chair
David Fielding MD
Australia, Treasurer
Naofumi Shinagawa,
MD
Japan,
Secretary General
Philippe Astoul, MD
France, President
WCBIP 2022
Menaldi Rasmin, MD
Indonesia, President
WCBIP 2024
STAFF
Michael Mendoza
General Manager
Judy McConnell
Administrator
Kazuhiro Yasufuku
Newsleer Editor-in-
chief
P A G E 2
Arcial Intelligence (AI) is not a novel concept. The
word “Arcial Intelligence” was coined by John
McCarthy in 1956, and the rst general-purpose
mobile robot was developed in 1969. The rapid
growth in technology soon created “Super Blue,” the
“supercomputer,” which defeated the world chess
champions.
AI is a type of computer science used to create intel-
ligent machines that recognize human speech and
objects and learn, plan and solve problems like hu-
mans.
AI can be understood in many ways depending on
one’s perspecve, as described below by some
world experts and leaders in the eld.
• AI is just math” - mulple computaons that are
the basis of AI are also where the technology faces
limitaons. Jana Eggers, the CEO of Nara Logics
• AI is just soware. “There’s no bright line sepa-
rang AI soware from any other kind of computer
soware,” Michael Liman, a computer science pro-
fessor at Brown University.
• The potenal of AI lies in its ability to learn, and
its learning from humans. Mikhail Naumov, co-
founder, president, and CSO of Digital Genius.
• Simply put, humans should be focused on teach-
ing machines, so that machines can focus on exe-
cung against jobs that are too big for humans to
process.” J.J. Kardwell, CEO/co-founder of Ever
String
In the eyes of some world experts of technology,
such as Elon Musk, CEO of Tesla, AI is a double-
edged sword. The potenal of AI is fundamentally changing
just about any aspect of our lives is so profound and self-
perpetuang that the threat of AI geng out of human
control makes him say that “AI is a fundamental risk to the
existence of human civilizaon.”
AI in medicine has been growing by leaps and bounds in all
facets, including diagnoscs, therapeucs, research, device
development, and drug development. Watson, the infa-
mous supercomputer, can diagnose thousands of diseases
with extreme expediency and accuracy. Numerous medical
organizaons now use it. Google’s “AI Rena Doctor” can
examine rena scans and diagnose diabec renopathy.
AI has also played a crucial role in the growth of Interven-
onal Pulmonology (IP) over the years. The below examples
will highlight some revoluonary AI-based developments in
IP.
• LungVision system (Body Vision Medical LTD, Israel) is a
novel technology that integrates pre-procedural CT imaging
into augmented uoroscopic images, presenng real-me
visualizaon of the airways and locaon of the pulmonary
lesion during transbronchial navigaon and biopsy. It ena-
bles lesion tracking during breathing movement and im-
proves lesion localizaon and diagnosc yield. LungVision
may provide equivalent diagnosc outcomes to tradional
ENB plaorms at a fracon of the cost.
• Opcal-based navigaon systems (such as SIRIO,
MASMEC S.p.A., Modugno, BA, Italy) perform Lung Thermal
Ablaon (LTA). Procedural planning, monitoring, and lesion
targeng are generally performed with the help of CT.
More recently, the implementaon of C-arm cone-beam CT
(CBCT) technology has introduced a new image guidance
strategy. Navigaon systems emerge as a valid tool to re-
duce procedural mes and administraon of radiaon dos-
es, allowing electromagnec, opcal, or hybrid tracking of
the devices used during intervenons and their real-me
visualizaon in a model obtained from a previously ac-
quired CT scan. In a recent study published in (1) opcal-
based navigaon system, SIRIO was shown to be an e-
cient tool to perform CT-guided LTA, displaying a signicant
reducon (p < 0.001) in the number of required CT scans,
procedure me, and paents’ radiaon exposure.
• A computer-aided diagnosis (CAD) system is a machine
learning texture model for classifying lung cancer subtypes
using preliminary bronchoscopic ndings is a CAD system.
This CAD system can disnguish cancer types to achieve an
W A B I P N E W S L E T T E R
P A G E 3
beer than the expert group.
In conclusion, AI has been advancing exponenally in every
walk of life, from essenal day-to-day funcons of turning on
a cell phone to ying ghter jets thousands of miles away
without a pilot. From human surveillance, nancial modeling,
fake news, invasive social media, educaon to religious
preaching. AI in medicine has enormous potenal to diagnose,
track, treat, and cure diseases. Like any other technology in
the past, it depends on how we use it.
References:
1. Laimer G et al. Biology. 2021 Jul; 10(7): 644
2. Feng PH et al. Med Phys. 2018 Dec; 45(12):5509-5514
3. Way TW et al. Med Phys. 2009 Jul; 36(7): 3086–3098
4. Cui S al. Scienc Reports. 2020 10:13657
5. Zhi X et al. Front Oncol. 2021 May 31;11: 673775
objecve diagnosis. A study (2) collected broncho-
scopic images of 12 adenocarcinomas and ten
squamous cell carcinoma paents. The images
were transformed from a red-blue-green (RGB) to a
hue-saturaon-value (HSV) color space to obtain
more meaningful color textures. A predicon mod-
el of malignant types was established by combining
signicant textural features (P < 0.05) in a machine
learning classier. The performance of the CAD
system achieved an accuracy of 86% (19/22), sensi-
vity 90% (9/10), specicity 83% (10/12), posive
predicve value 82% (9/11), and negave predic-
ve value 91% (10/11) in disnguishing lung cancer
types.
• Another CAD system of a pulmonary nodule on
CT scans led to improved classicaon perfor-
mance with nodule surface features. A fully auto-
mated system was designed to segment the nodule
from its surrounding structured background in a
local volume of interest (VOI) and extract image
features for classicaon. A study (3) demonstrat-
ed that the CAD-based segmentaon and feature
extracon techniques are promising for classifying
lung nodules on CT images.
• AI is showing rapid advantages and excing
achievements in diagnosc imaging and evaluaon.
Many novel deep neural network-based systems
have demonstrated the potenal for use in the
proposed technique for helping radiologists im-
prove nodule detecon accuracy with eciency
and cost-eecveness. In a study (4), 39,014 chest
low dose CT screening (LDCT) cases were retro-
specvely collected. The diagnosc performance of
the deep learning (DL) algorithm was evaluated in
the mul-center validaon set and the external
test set (LUNA). In total, 11,840,536 and 134,985
LDCT images obtained from 39,014 imaging studies
were assigned to the training set and validaon
set, respecvely. The DL model showed a high de-
gree of agreement with the reference standard.
• In a study (5) of Automac Image Selecon
Model Based on Machine Learning for Endobron-
chial Ultrasound Strain Elastography Videos, the AI-
based technology showed 78.02% to 83.52% accu-
racy in diagnosing malignant from benign medias-
nal and hilar lymph nodes based on the relave
sness of the ssue. This accuracy was much
higher than the trainee group and equal to or
W A B I P N E W S L E T T E R
P A G E 4
Technology Corner
Augmented Imaging for Peripheral Bronchoscopy
Introducon:
Tradional guided bronchoscopy modalies include standard uoroscopy, radial ultrasound, and electromagnec guidance.
Despite evolving technology and tools, biopsy yields have remained around 70% in most studies. Roboc bronchoscopy
plaorms have emerged as opons for peripheral bronchoscopy with the promise of beer yields due to their ability to
beer reach peripheral regions of the lung, along with the ability to maintain vision during sampling, all while having beer
p stability especially in the case of eccentric lesions sampling. Despite this promise, the rst published studies showed
only modest improvement in yield (1,2). There are mulple reasons cited for subopmal yield; these include poor perfor-
mance of biopsy tools, local atelectasis that develops during the procedure, and CT-body divergence. Using cone beam CT
(CBCT), invesgators found that there can be signicant divergence in nodule locaon between the pre-procedure CT imag-
ing and lung during procedure (3). This divergence is largest in the lower lobes, and can be greater than 15mm in distance,
easily enough to rend a biopsy aempt spuriously away from the intended target, potenally resulng in a falsely negave
result. Accepng tool performance as a constant, it appears that accurate targeng of the nodule is therefore a major de-
terminant of yield. Up unl recently, the only surrogates of accurate targeng were uoroscopy and radial ultrasound
(rEBUS). Standard uoroscopy can only be employed when the nodule is visible, and rEBUS is mainly helpful when the le-
sion is concentrically posioned around the airway. Further, neither rEBUS or uoroscopy can provide accurate assess-
ments of distance and angular relaonships of the tool with the lesion. The emergence of CBCT has overcome these imped-
iments with detailed imaging and 3D reconstrucon, oering real insight into tool-nodule relaonship. Unfortunately, CBCT
is not readily available at all instuons and is expensive. As a result, other imaging modalies have been developed to
achieve the same goals. These modalies use enhanced uoroscopy images, and thus are less costly and use a much small-
er space footprint within the bronchoscopy suite, and therefore allow for broader adaptaon by proceduralists.
Background:
Augmented imaging refers to any real me imaging (ie uoroscopy) being augmented by other imaging sources (ie CT, ul-
trasound, etc). Mulple imaging modalies can then be fused (“image fusion”) simultaneously. Though imaging sources can
be real-me or historic, the augmentaon is real me. Currently there are several technologies on the market that achieve
augmented imaging, however only one, LungVision
TM
(Body Vision Medical INC, NY) uses intraoperave tomography to aug-
ment real-me uoroscopy. The resultant augmented uoroscopic imaging contains an overlay of both the airway pathway
Joseph Cicenia, MD
Cleveland Clinic
W A B I P N E W S L E T T E R
P A G E 5
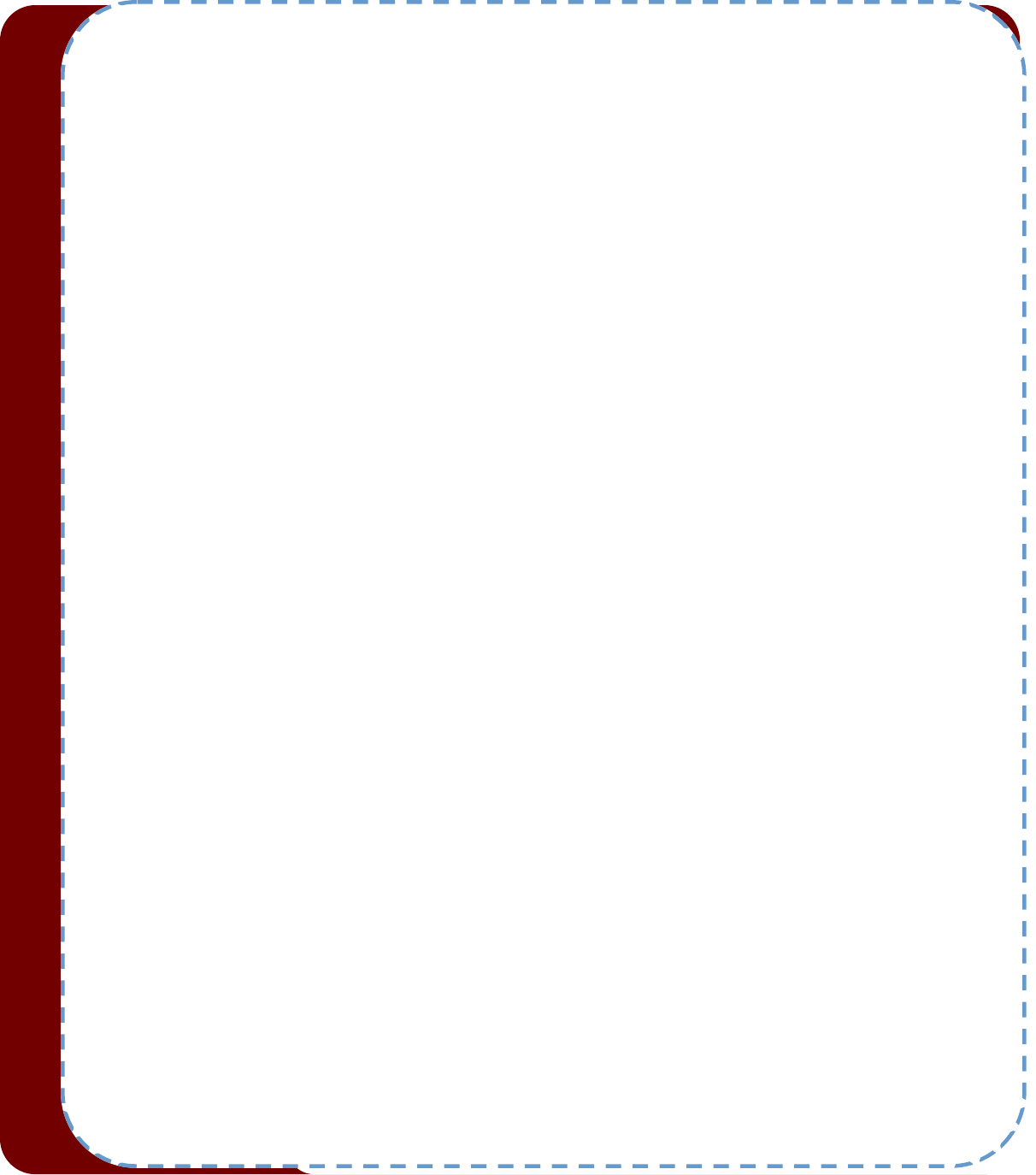
to the lesion, and the lesion itself (see Fig 1).
Clinical Applicaon:
How we do it
Aer the paent is anesthezed, a series of uoroscopy images are performed to achieve CT-body registraon. Then, a
uoroscopy spin (typically -50° to +50°) is performed with the nodule at isocenter. Aer images are reconstructed tomo-
graphically, nodule locaon is updated and the overlay appears for navigaon to begin. Once navigaon to the nodule is
completed, another uoroscopy spin is performed which gives 3D representaon of the nodule with the catheter and/or
biopsy tool, and nodule locaon correcons are performed if needed (see gs 2,3). Catheter and/or biopsy tool locaon
correcons can be made at this me, if necessary, and another spin can be performed to re-image tool-nodule arculaon.
Once the tool locaon and projected trajectory is deemed to be adequate, biopsies are done, again using augmented imag-
ing. Though uoroscopy use is increased during these procedures, cases have shown average doses around 250 mGy, about
one tenth that of a cardiac catheterizaon.
Accuracy
The applicaon of real-me imaging and localizaon during navigaonal bronchoscopy has promise, and has been suggest-
ed by results from mulple studies. For example, studies that have used advanced navigaonal technologies in conjuncon
with real-me CBCT imaging have suggested the addive nature of these technologies compared to their respecve individ-
ual yields (4). Indeed, published studies using LungVision have shown high localizaon rates (90-95% using rEBUS and
CBCT), albeit with earlier versions of the technology, with yield ranging between 77 and 84% (5,6). This compares well to
published rates of roboc bronchoscopy localizaon (85-90% range) and yield (1,2). It will be interesng to see if merging of
augmenng imaging (either CBCT or LungVision) with roboc bronchoscopy will result in higher yield procedures; studies
are commencing to evaluate this further.
Conclusion
It is apparent that augmented imaging can play an important role in peripheral bronchoscopy. Though this can be achieved
with CBCT, these systems are expensive, have large space footprints, and may be dicult to have access to. Using alterna-
ve technologies, such as LungVision, can provide similar imaging with standard uoroscopy equipment, and can be easily
incorporated into the bronchoscopy suite. Further research into the plaorm itself, as well as combining this plaorm with
roboc technologies is underway.
References:
1. Kalchiem-Dekel et al. Chest. 2021 Aug 9;S0012-3692(21)03625-4
2. Chaddha et al. BMC Pulm Med 19, 243 (2019)
3. Pritche et al. J Bronchology Interv Pulmonol. 2021 Jan 1;28(1):10-20
4. Verhoeven et al. J Bronchology Interv Pulmonol. 2021 Jan 1;28(1):60-69
5. Pritche,et al. J Bronchology Interv Pulmonol. 2021 Apr 1;28(2):107-115
6. Cicenia et al. J Bronchology Interv Pulmonol. 2021 Apr 1;28(2):116-123
W A B I P N E W S L E T T E R
P A G E 6
Figure 1: Augmented imaging overlay with pathway and nodule.
Figure 2: Tomographic reconstrucon of nodule with
catheter leading into it.
Figure 3: 3D reconstrucon of the nodule-catheter
relaonship.

Tips from the Experts
P A G E 7 V O L U M E 1 0 , I S S U E 1
Introducon
Diagnosc procedures for sampling peripheral pulmonary lesions (PPL) have developed remarkably over the last two decades as more lung
nodules are being idened due to liberalized lung cancer screening guidelines, increasing prevalence of chronic lung disease, and improve-
ments in advanced chest imaging. Two such plaorms include electromagnec navigaon bronchoscopy (ENB) and roboc assisted bron-
choscopy (RAB), which overall have improved diagnosc yield for PPL sampling [1-6].
Indicaons
When using ENB or RAB, proprietary planning soware uses computed tomography (CT) of the chest with thin-slice protocol (1 mm cuts)
obtained during full inspiraon to build a virtual bronchoscopic image of the tracheobronchial tree. A computer-generated pathway from
the target lesion to a more centrally located airway is constructed, and the bronchoscopist can manually adjust and extend the mapped
pathway as needed. This pathway serves as a guide to the target lesion during bronchoscopy. During the procedure, the main plaorm gen-
erates an electromagnec eld around the paent’s chest. This enables synchronizaon of a probe or sensor with the CT scan, and the bron-
choscopist can track the synchronized probe or sensor while navigang through the airways.
During the pre-procedural planning phase, the bronchoscopist may adjust or extend the computer-generated pathway by selecng and add-
ing points along visible airways on the CT chest from the target lesion to the central airway. This is oen known as the “bronchus sign”,
which is dened as the presence of an airway leading directly to a pulmonary lesion. The presence of a “bronchus sign” has been associated
with an improvement in diagnosc yield. In a meta-analysis of 2,199 lesions, the diagnosc yield was reported as 74.1% when a “bronchus
sign” was present vs 49.6% in its absence [7]. Seijo and colleagues also reported an increased diagnosc yield of PPL sampling with ENB with
the presence of a “bronchus sign” (79% vs 31%) [8]. Likewise, the diagnosc yield of PPL sampling by RAB was reportedly increased with the
presence of a “bronchus sign” in a mul-center study by Chaddha and colleagues (78.3% vs 54.1%) and in the BENEFIT trial (75.0% vs 72.7%)
[2,4]. The large mul-center NAVIGATE trial evaluang the ENB system by Medtronic also demonstrated that the presence of a “bronchus
sign” was associated with higher diagnosc yield (78.3% vs 67.1%) [9].
However, prior studies have reported that up to 40% of paents lack a “bronchus sign” when undergoing navigaonal bronchoscopy espe-
cially in paents with emphysema, in which the resoluon of the CT chest is subopmal for idenfying peripheral airway walls [8,10-12].
Therefore, alternave strategies in these sub-group of paents are necessary to provide navigaon precision. Recognizing that vessels, lym-
phacs and airways are oen adjacent in the bronchovascular bundle, in paents where a vessel is seen leading to the target nodule there
should also be a conguous airway which may not be seen on the CT due to the lack of contrast between the peripheral bronchi and sur-
rounding lung parenchyma (Figure 1). The evidence supporng vessels as a surrogate for a “bronchus sign” on CT is well corroborated by
developmental biology as blood vessels develop at the same me as airways; and specically, the pulmonary arteries run alongside the air-
ways and the pulmonary veins show a similar branching paern to the arteries [13,14]. Therefore, a “vessel sign”, dened as a vessel leading
directly to a target lesion, can be used as a surrogate for mapping during pre-procedural planning when a “bronchus sign” is absent (Figure
1).
Using the “Vessel Sign” for Pre-procedural Planning in Navigaonal and
Roboc Bronchoscopy
Sepmiu Murgu, MD
The University of Chicago
Elliot Ho, DO
Loma Linda University
Tips from the Experts
P A G E 8 V O L U M E 1 0 , I S S U E 1
Planning
During the pre-procedural planning phase, the CT chest is rst imported into the planning plaorm. Once segmentaon is complete, the
bronchoscopist idenes and marks the target lesion. The proprietary soware then constructs a computer-generated pathway towards the
target lesion, which may be incomplete and require manual adjustment. By appreciang the airways and vessels leading to the target lesion
on pre-procedural CT, the bronchoscopist can manually adjust and extend the computer-generated pathway by tracing over and adding
points along such airways and vessels from the target lesion towards the central airway. In our experience with ENB and RAB, we have had
success using the “vessel sign” as a backup pathway when the registraon CT scan lacked a clear “bronchus sign” (Figure 2).
It should be noted, however, that the advancement of navigaonal technology for PPL sampling is not a replacement for experience and
thoughul review of imaging and airway anatomy. Successful planning of a pathway for PPL sampling using navigaon plaorms requires
appropriate understanding of the tracheobronchial anatomy.
Sampling
Airway inspecon using a convenonal white light bronchoscope is typically performed prior to convenonal ENB and RAB to rule out central
endobronchial lesions and aspirate secreons if present. Navigang to the target lesion via guided bronchoscopy using the virtual pathway
created on the pre-procedural planning soware is then used (Figure 2). Before sampling the target lesion, successful localizaon to the tar-
get lesion is demonstrated based on feedback from the navigaon system and typically conrmed with a second method of visualizaon (e.g.
r-EBUS, uoroscopy, cone beam CT, augmented uoroscopy) (Figure 2). Once localizaon is conrmed, endoscopic tools are passed via the
working channel of the bronchoscope to sample the target lesion. The presence of rapid onsite cytology evaluaon (ROSE) allows for real-
me conrmaon of whether lesion material is obtained. While ROSE provides value regarding ssue adequacy for molecular proling, it is
unclear whether the use of ROSE aects the diagnosc accuracy for sampling parenchymal lesions [9].
Quality Control
Any soware that uses a CT performed at total lung capacity will lead to CT-body divergence, in which the true locaon of a PPL is not always
consistent with the navigated virtual target, under the condions of general anesthesia. This is due to the dierences in lung volume at the
me of the planning CT scan and when the actual procedure is performed. This is especially true when the target lesion is in the lower lobes,
in which atelectasis is more prevalent during general anesthesia and there is more diaphragmac excursion. Real-me imaging has been the
emphasis of more recent technology to improve PPL localizaon.
Radial EBUS has been shown to conrm proper placement of the sampling tools and verify its proximity to the target lesion, increasing diag-
nosc yield [1,10,15]. Prior to the introducon of RAB, the paern of r-EBUS image usually aected diagnosc yield, in which a higher yield
was noted when concentric r-EBUS views are obtained (84%) as compared with eccentric r-EBUS views (48%) [16]. The alignment of the bron-
choscope working channel in relaon to the target lesion can be adjusted based on the radial EBUS view. Eberhardt and colleagues reported
that the combined use of r-EBUS along with ENB improved diagnosc yield of up to 88% as compared with either technology alone [17]. With
RAB, some studies show that the yield is not aected by the r-EBUS paern [2,4].
Digital tomosynthesis via augmented uoroscopy (AF) with convenonal C-arm and cone-beam computed tomography (CBCT) aempt to
correct for CT-body divergence and provide real me feedback of the bronchoscope or tool locaon. This is in eort to allow for ne adjust-
ments of ENB or RAB to beer align the working channel with the target lesion and assist with redirecng sampling tools as needed, increas-
ing localizaon success and potenally diagnosc yield [3,18-20]. To date, there is no evidence, however, that these technologies signicantly
improve diagnosc yield when compared with RAB technology alone.
Conclusion
Advancements in navigaonal bronchoscopy and advanced imaging techniques have empowered bronchoscopists to access the periphery of
the lung with more condence and increasing accuracy. As newer advancements in navigaonal bronchoscopy and soware connues to
develop, the ability of the bronchoscopist to recognize and plan pathways to the target lesions is even more important.
The “vessel sign” can be used as a potenal surrogate for the “bronchus sign” when mapping a pathway for navigaonal bronchoscopy and
an airway leading to the lesion cannot be visualized. Potenally, the use of the “vessel sign” during pre-procedural planning may be able to
improve the rate of navigaon success for ENB and RAB procedures that lack a “bronchus sign”. Studies are needed to conrm the validity of
using the “vessel sign” for pre-procedural planning during navigaonal bronchoscopy and clarify its eect on outcomes including rate of local-
izaon success, diagnosc yield, and complicaon rates.
Tips from the Experts
P A G E 9 V O L U M E 1 0 , I S S U E 1
References
1. Folch EE et al. Chest. 2020 Oct; 158(4):1753-1769.
2. Chen AC et al. Chest. 2021 Feb; 159(2):845-852.
3. Pritche MA et al. J Bronchology Interv Pulmonol. 2018 Oct; 25(4):274-282.
4. Chaddha U et al. BMC Pulm Med. 2019 Dec; 11;19(1):243.
5. Chen AC et al. Ann Thorac Surg. 2018 Jul; 106(1):293-297.
6. Chen AC et al. Respiraon. 2020 Jan; 99(1):56-61.
7. Ali MS et al. Ann Am Thorac Soc. 2018 Aug; 15(8):978-987.
8. Seijo LM et al. Chest. 2010 Dec; 138(6):1316-21.
9. Folch EE et al. J Thorac Oncol. 2019 Mar; 14(3):445-458.
10. Ali MS et al. Respirology. 2017 Apr; 22(3):443-453.
11. Brownback KR et al. J Bronchology Interv Pulmonol. 2012 Apr; 19(2):91-7.
12. Hsia DW et al. J Bronchology Interv Pulmonol. 2012 Jan; 19(1):5-11.
13. Hall SM et al. Am J Respir Cell Mol Biol. 2000 Aug; 23(2):194-203.
14. Loosli CG et al. Am Rev Respir Dis. 1959 Jul; 80(1, Part 2):5-23.
15. Kurimoto N et al. Chest. 2004 Sep; 126(3):959-65.
16. Chen A et al. Ann Am Thorac Soc. 2014 May; 11(4):578-82.
17. Eberhardt R et al. Am J Respir Crit Care Med. 2007 Jul; 176(1):36-41.
18. Aboudara M et al. Respirology. 2020 Feb; 25(2):206-213.
19. Cicenia J et al. J Bronchology Interv Pulmonol. 2021 Apr; 28(2):116-123.
20. Casal RF et al. J Thorac Dis. 2018 Dec; 10(12):6950-6959.
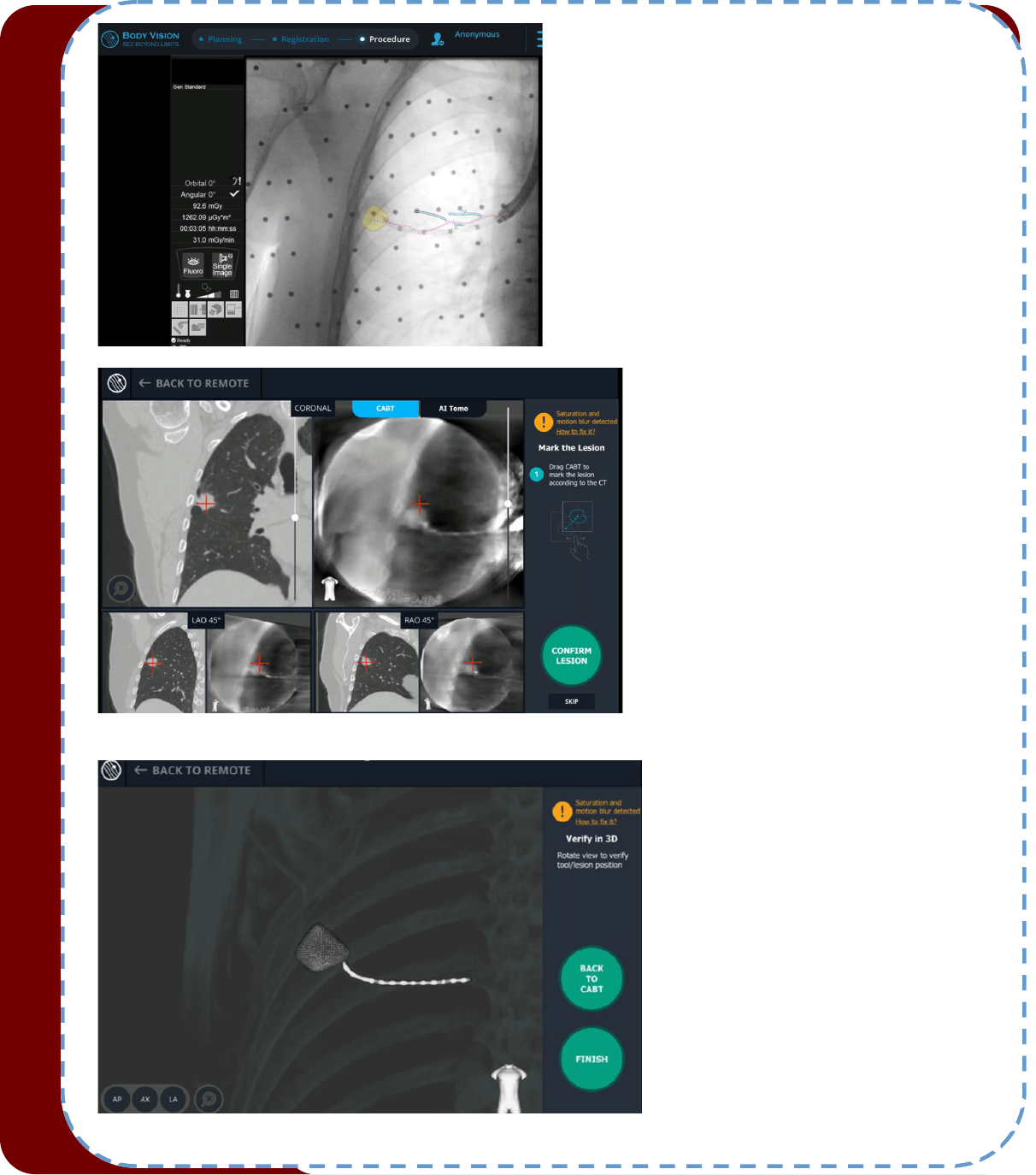
Figure 1. The “Vessel Sign”. CT image in the axial
plane showing a subsolid peripheral nodule
(yellow arrow) without a bronchus sign (A). How-
ever, a pulmonary artery branch was idened
(blue arrow) leading to the nodule (B).
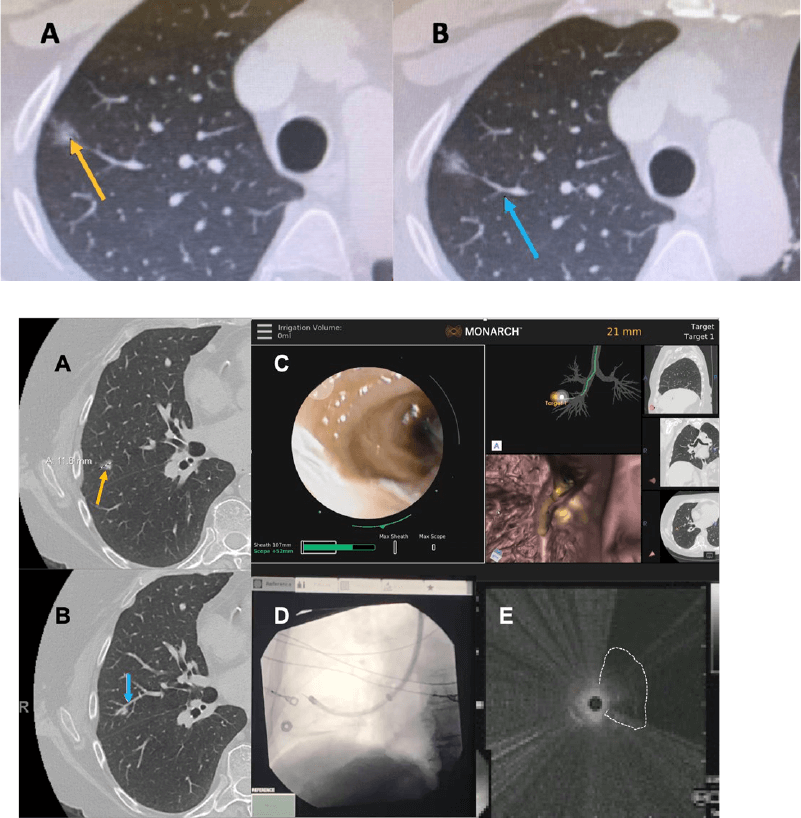
Figure 2. Using the “Vessel Sign” for Lung Nodule Sampling
with Roboc Bronchoscopy. The nodule (yellow arrow) is
seen in the lateral segment of the right middle lobe (A). A
vessel (blue arrow) is seen leading to the nodule and was
used for manual planning (B). The roboc bronchoscope is
advanced to the target lesion and parked proximal to the
lesion while vision is sll maintained by air insuaon (C).
Fluoroscopy shows the sheath, scope and radial EBUS probe
(D). Radial EBUS image shows a small eccentric nodule
(highlighted by the doed line) conrming successful navi-
gaon (E).
Humanitarian News
W A B I P N E W S L E T T E R P A G E 10
Ethical Issues about Waiving Intellectual Property Protecons for COVID-19
Vaccines
In 1796 Edward Jenner developed the rst vaccine by taking material from cowpox lesions on a cow maid and injecng it
into an eight-year-old boy. Several weeks later, he injected the boy with live smallpox, with no ensuing infecon. The World
Health Organisaon (WHO) has only ever declared two diseases exnct: the cale disease rinderpest, and one human dis-
ease, smallpox. Both were the result of massive vaccinaon drives and global campaigning.
However, the road to eradicaon was not an easy one. The technical and sanitary challenges (parcularly in tropical coun-
tries) seemed impossible to be overcome. In the 1950s, Leslie Collier developed a freeze-dried vaccine. In the following dec-
ade, Benjamin Rubin of Wyeth Laboratories designed the bifurcated needle, which made easier a reliable vaccinaon. These
technical developments but mainly the decision to waive patents and royales on the needle and vaccine, enabled the WHO
to launch its 1966-1977 campaign to eradicate smallpox globally and aer 14 years of careful searching and contact tracing
and millions of vaccines one of the biggest killers in history was eradicated.
In the last century, few diseases have reached a global devastang eect on mortality in the form of outbreaks of major epi-
demics. Probably because of that, even when vaccinaon (together with hygiene and sanitaon measures) have dramacally
improved life expectancy, the concept of vaccines as a public good was slowly fading.
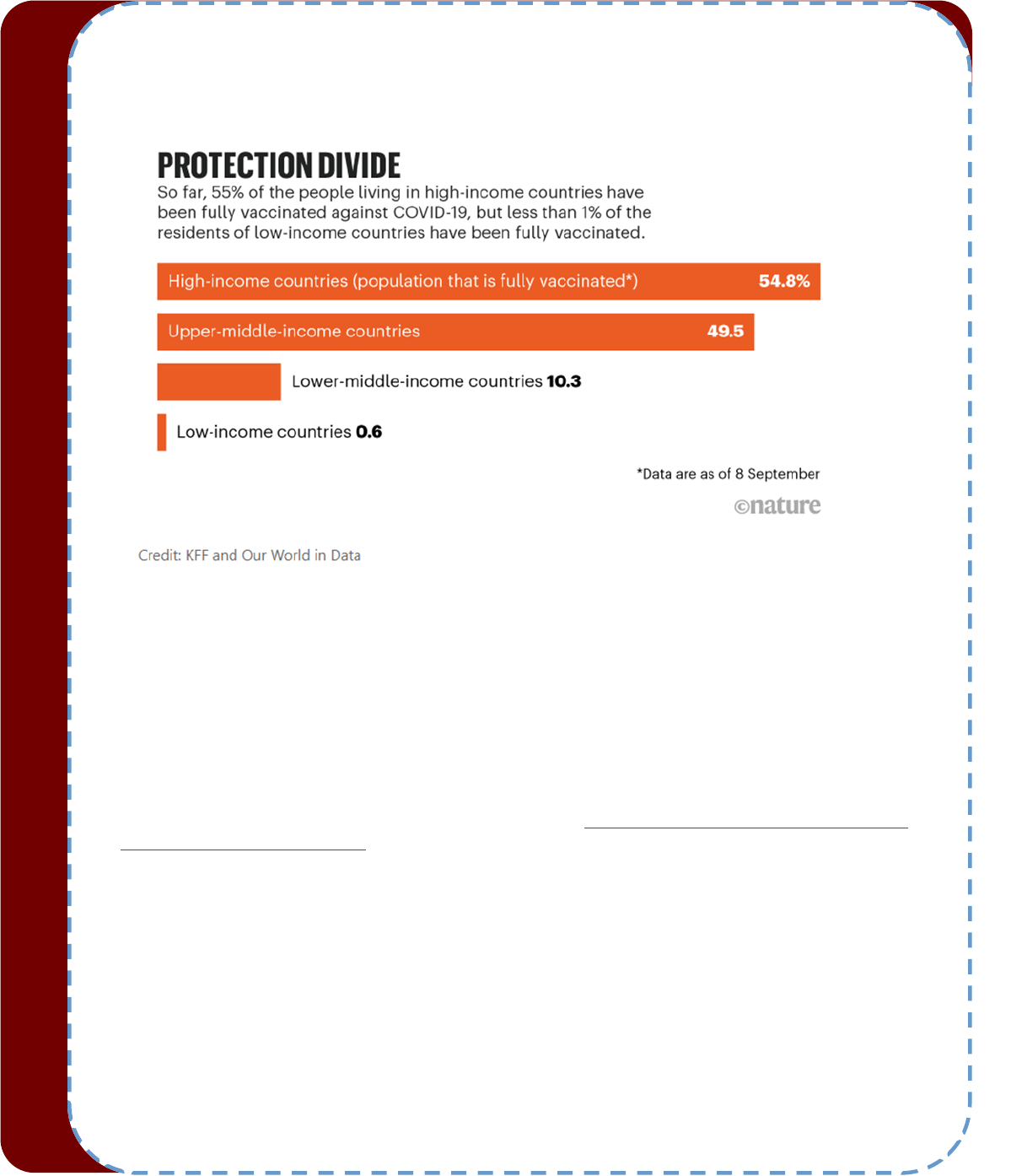
But now that vaccine inequity leaves lower income countries – many of them in Africa – at the mercy of COVID-19, the ethi-
cal discussion about the moral duty of developed naons for waiving patents to vaccinate more quickly the global south has
become not only necessary but also urgent.
WHO has set a global target of 70 per cent of the populaon of all countries to be vaccinated by mid-2022, but to reach this
goal a more equitable access to vaccines will be needed. And this is not a necessity only for the underserved communies
with insucient access to vaccinaon, this is an urgent need for the whole world. As Dr Tedros Adhanom Ghebreyesus, the
Director-General of the World Health Organizaon (WHO) said vaccine equity was “not rocket science, nor charity. It is smart
public health and in everyone’s best interest.”
The ethical principles guiding the distribuon of vaccines should be considered, especially for those at high risk. It is well
known that from late December, 2020, countries started vaccinang their populaons, however, those millions of available
doses were concentrated in high-income countries, which have purchased 54% of secured doses but which account for only
19% of the global populaon.
The right balance between private prots and public health is not a new issue but a long-running debate. Many experts and
humanitarian NGOs contend that World Trade Organizaon (WTO) rules on intellectual property (IP) limit poor countries’
access to crical medicines. On the other hand, defenders of conceiving essenal medicines as any other commodies, point
that the IP rules are needed to incenvize drug makers.
Unfortunately, ethical principles in health policy have oen been neglected when they have concerned vulnerable groups,
with the distribuon of life-saving drugs judged too expensive and unsustainable and the recipients considered unworthy.
Lack of foresight, incenves, and polical will has caused a serious violaon of the principle of jusce and the consideraon
of access to health care as a universal human right.
But beyond the general principle that ethical allocaon of every kind of health care resources is crucial for the principle of
Humanitarian News
W A B I P N E W S L E T T E R P A G E 11
jusce, the massive and rapid spread of COVID-19 epidemic and the associated high rates of mortality have
turned necessary an urgent debate about an essenal moral queson: is it ethically acceptable to uphold vaccine patents
during a global shortage?
The naturalizaon that low-income countries should and can spend substanally less on saving the lives of their vulnerable
groups, sadly indicates that the value of one's life is linked to their country's income. And during a dramac emergency as a
lethal but potenally preventable disease, it has shone a harsh spotlight on the fact that the global community accepts that
the lives of those in low-income countries are worth less than the lives of those in high-income countries. The valuaon of
life solely based on where an individual lives generates unethical guidelines about health policies that negate an individual's
human right to health.
The WTO’s Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) commits members to guaranteeing
twenty-year patents and safeguards for copyrights, trade secrets, and industrial designs, prevenng companies other than
the inventors from manufacturing those medical products. Based on warranng the access to crical medicines globally, in
late 2020, a group of low-income countries led by India and South Africa proposed that the WTO temporarily waive IP pro-
tecons for vaccines unl most of the world’s populaon gets immunizaon. This would allow other companies, including
those in developing countries, to make generic brands of exisng vaccines. The U.S. and E.U., as well as countries including
the UK, Japan, and Australia among others, opposed the proposal while over 100 other countries have supported the waiver.
In May 2021, the Joe Biden administraon reversed course and announced its support for a vaccine IP waiver. Not much
later, a coalion of developing countries pressing for the waiver, submied a new proposal quite similar to the rst that
specied that the waiver would apply to pandemic-related “health products and technologies,” and advising the waiver
should last for at least three years.
As a result of those events, a heated debate has been seled worldwide. But two dierent aspects need to be dierenated
about this issue. On the one hand, controversy may exist about the ecacy of the waiver in its goal of raising access to Covid
-19 vaccines in poor countries, based on the dicules of companies in developing countries to learn from the original pro-
ducers how to produce eecvely in the short run and the lack of vaccine producon facilies and technology. It is argued
that the absence of patents will do lile to remedy the structural deciencies that impede a quickly expanding producon
capacity in developing countries on the scale and speed needed to a large scale producon that solve the access problem.
But, although the argument that the patent waiver will, by itself, do lile to address the short-run access problems is proba-
bly right, a very dierent issue is the ethical legimacy of upholding the patents and deliberately denying access to some
populaons in the pursuit of prots or in order to give priority to certain groups.
Analyzing the subject strictly from a moral point of view one could apply the argument that vaccine patent waivers could
allow other countries to produce generic copies and increase the global supply of vaccines and that the increase of vaccines
availability could save lives and decrease the prevalence of future COVID variants, which is threatening to prolong the pan-
demic.
From a Kanan perspecve, the answer seems crystal clear. Maintaining patents violates the principle of benecence, doing
good for others, by deliberately refusing to help countries in dire need. It also violates the principle of non-malecence,
avoiding harm to others, as patents can discourage innovators from other countries from developing a novel vaccine for fear
of copyright suits.
All the social actors are also moral agents including policy makers, CEOs of mulnaonal companies and scholars or inven-
tors. Being as they are human beings, they must face every day the same queson we all human face: is my behavior morally
correct, am I honouring my own humanity? We know that all persons, regardless of rank or social class, have an equal intrin-
Humanitarian News
W A B I P N E W S L E T T E R P A G E 12
sic worth or dignity. Human dignity is an innate worth or status that we did not earn and cannot forfeit. Rather, we must
strive to make our individual choices worthy of this moral standing, which elevates us above animals and mere things. Kant
expresses the principle of humanity (PH) as follows: “Act in such a way that you treat humanity, whether in your own person
or in the person of any other, never merely as a means, but always at the same me as an end”. It is a principle, Kant holds,
that would describe the conduct of fully raonal beings toward themselves and each other, so it is a principle that should
describe the conduct of human beings toward themselves and each other.
That respect for human dignity requires that everyone fulls his or her duty. In The teleological argument, Kant disnguishes
among: a) the case in which a person clearly acts contrary to duty; b) the case in which a person's acons coincide with duty,
but are not movated by duty; and c) the case in which a person's acons coincide with duty because he or she is movated
by duty. And Kant (and much of the post-Kanan philosophy) explicitly expresses that our acons only have moral worth and
deserve esteem when they are movated by duty. Those consideraons led to the construcon of the Categorical Impera-
ve. Kant characterized the CI as an objecve, raonally necessary and uncondional principle that we must always follow
despite any natural desires or inclinaons we may have to the contrary. Thus, the supreme formal principle of Kant’s ethics
is: “Act only on that maxim through which you can at the same me will that it should become a universal law.”
And so the queson is: can any human being wish that the rule that nancial prot must be always preserved (even at the
cost of hundreds of thousands of preventable deaths) become a universal law? And if not: is any reward treasured enough to
choose acons against our raonal duty and consequently with no moral worth and that does not deserve any esteem and
deny our own humanity?
Crics of the proposal argue that a waiver would discourage future innovaon. The technology ulized by the Pzer-
BioNTech and Moderna vaccines were only possible through years of research and development from the public and private
sector. If companies have no prot incenve to create these new health care products, investments in the industry drop and
this could lead to a decline in new technologies. It has also been menoned that it would create a potenal disadvantage for
US companies if allowing China and other rival countries to obtain essenal IP. The primary basis for this arguments is that
the prots IP generates are essenal to spur innovaon and discovery which in turn, advance society’s interests. The ques-
on is, even if it were true: how much nancial incenves are needed, how much money does it take? In 2021, Pzer/
BioNTech will make 15–30 billion US dollars from COVID-19 vaccine sales, Moderna 18–20 billion US dollars, and Johnson &
Johnson 10 billion US dollars. Could these companies earn less and the incenve to innovate remain intact?
Helping others may always have a cost. Even Kant menons that helping others is “an imperfect duty”, and in his concepon,
an imperfect duty allows exibility—benecence is an imperfect duty because we are not obliged to be completely bene-
cent at all mes, but may choose the mes and places in which we are. Big companies may argue (and do argue) that they
are not charitable organizaons, that looking for the highest possible prots is a legimate aim and that they can choose
how and when help others. However, as the notorious contemporaneous philosopher Peter Singer has shown in his famous
book “The life you can save”, that “exibility” is far from being unlimited.
Singer exemplies that situaon in the simple but categorical philosophical experiment of the drowning child. On your way
to work, you pass a small pond. You see a child splashing about in the pond and by geng closer, you see that he is ailing
about, unable to stay upright or walk out of the pond. There is no one else around. If you don't wade in and pull him out, he
seems likely to drown. Wading in is easy and safe, but you will ruin the new shoes you bought only a few days ago, get your
suit wet and muddy and you will be late for work. What should you do? Predictably, most of people respond that you should
save the child. The premise behind that well known story is: if it is within our power to prevent something bad from happen-
ing, without thereby sacricing anything of comparable moral importance, we ought, morally, to do it. In a similar way, we
may ask ourselves (beyond the praccalies of the real impact of the waiver of patents) if thousands and thousands of
Humanitarian News
W A B I P N E W S L E T T E R P A G E 13
deaths and the consequences of collapsed economies are not worthy of sacricing some minor nancial prots.
The essenal feature of capitalism is the move to make a prot and one of its founding pillars is self-interest, through which
people act in pursuit of their own good, without regard for sociopolical pressure. Nobody expects that neither entrepre-
neurial businesses nor big rms resign their purpose of making prot or work for losing money. But the queson is: are the
big pharma companies that develop and manufacture vaccines at the risk of losing money?
Between 2000 and 2018, 35 big drug companies received a combined revenue of $11.5 trillion, with a gross prot of $8.6
trillion. The median net income margin reported by 35 pharma companies between 2000 and 2018 was almost twice as high
as it was for the 357 non-pharma companies included in the comparison. Funding for pharmaceucal research and develop-
ment (R&D) is the result of a complex mix of private and public sources. Governments mainly support basic and early-stage
research. Such funding is made through direct budget allocaons, research grants, publicly-owned research instuons and
funding of higher educaon instuons. The pharmaceucal industry translates and applies knowledge generated by basic
research to develop products, and invests in large clinical trials required to gain market approval. The industry also receives
direct R&D subsidies or tax credits in many countries. But despite the pharmaceucal rms are substanally supported by
government subsidies, yet the price for most medical products is mulple mes the producon cost. In products whose
availability put lives of people at stake, “the invisible hand” of the market if far from being balanced, as the access to drugs
and medical technologies is not a maer of choice but of essenal need. Addionally, the huge eort made by the research-
ers is not a solitary endeavor. The thousands of volunteers that made the tesng needed for the approval of the new vac-
cines possible, the previous basic research on what the new developments are based, the pilots of planes and drivers of
trucks who transported the vaccines, the thousands of health care workers involved in the organizaon and implementaon
of the vaccinaon campaigns that did not take any addional prot, all of them were indispensable components of the net-
work required for the vaccines reach every single target subject.
The margins of prots of the big pharma companies has become a heated debate in many countries in the last years. Many
have quesoned that subsidies given by the governments come from the taxes paid by cizens including vulnerable groups,
and the deliberate decision to sell drugs at extremely high prices let those same vulnerable groups that support them by
taxes deprived of their right to health because they cannot aord them. In fact, although this year the rapid and eecve
development of COVID-19 vaccines improved substanally their popularity, for decades, few industries in the US have been
as unpopular as Big Pharma.
Many scholars and social and polical acvists trusted that new winds were arriving in the world economy as a reacon to
the many failures that a previously successful system as the capitalism is showing currently all over the world. Many of the
world’s eco-systems are on the edge of collapse, inequality increases persistently, and systemic racial and ethnic exclusion
disgrace every society on the planet. Even business leaders are voicing these opinions with crics to convenonal capitalism
and accepng that it is in urgent need of redempon. Ajit Ranade, president of Aditya Birla Group even said capitalism is
losing support because of its failure to address widening inequalies. In that sense, one of the challenges seemed to be a
renewal of the purpose of the rms—away from only maximizing shareholder value towards including ‘solving public prob-
lems protably and avoiding creang new problems’. It would allow the private sector to become an acve partner in cre-
ang a just and sustainable society. Many enthusiasc analysts saw an example of that in the inial commitment of Pzer to
provide ered pricing for middle-income countries while providing the vaccine for free in Africa. However, many of Pzer's
contracts requesng guaranteeing the company indemnity and forcing the governments to compensate for any adverse
eects of the vaccine, faded any hope to ensure ethical cosng.
Many conservave economists all over the world sll support the Milton Friedman’s theory that the social responsibility of
business is to increase its prots and that a corporaon is a morally neutral legal construct with maximising returns for
Humanitarian News
W A B I P N E W S L E T T E R P A G E 14
shareholders as its single purpose. But even with that self-centered understanding of business, nobody should deny the un-
matched value of a human life. The pandemic has transformed the discussions about the impact of inequalies, unfairness
and unethicalness from abstract speculaons to concrete daily pictures of human deaths. Figures, pictures and personal his-
tories hit us right in the face every day from the news and the social media. Addionally, the polical manipulaon of the
pandemic has created many obstacles for a raonal management of the epidemic. The vaccine development process has
been linked to elecon cycles in many countries, with polical leaders making not always accurate promises about the vac-
cine which reduced the trust that individuals have in the results of what appear to be rushed clinical trials. An-vaccine
groups have gained popularity increasing enormously their followership base since 2019. An irresponsible behavior of many
news media and the undeniable history of unethical exploitaon of vulnerable groups caused vaccine hesitancy in many pop-
ulaons in dierent countries, increasing the risk of death and suering from the disease.
The principle behind the campaign to temporarily waive IP protecon for COVID vaccines is that every country should have
the right to make its own vaccines during a pandemic. Waiver is surely not the only or even the best soluon to increase
access and the implementaon of the waiver engenders several intrinsic challenges. The tools and technologies required for
this purpose are currently owned by only a few pharmaceucal companies and probably not all countries would have on-site
pharmaceucal industries that can guarantee adequate protecve measures both for the technicians in the laboratories or
for the surrounding populaons. High safety levels for the associated biological risk are required and dicult to achieve. Na-
onal health surveillance procedures may not be as strict as desirable to monitor potenal risks and side eects. Producon
in condions of imperfect biological quality control could result in more adverse reacons. Obviously, loosening the grip of IP
protecons is not a miracle x, and there are many other barriers to a safer world. All of these are important arguments, and
need to be addressed. But they are not, in themselves, reasons for denying IP relief.
A study by the WHO Regional Oce for Europe and the European Centre for Disease Prevenon and Control (ECDC) es-
mates that 470 000 lives have been saved among those aged 60 years and over since the start of COVID-19 vaccinaon
rollout in 33 countries across the WHO European Region, not including lives saved by vaccinang people under 60 nor those
saved from the indirect eect of vaccinaon because of a reducon in transmission. Denying or delaying access to vaccina-
on costs lives, concrete singular lives with names and beloved ones. And no one more death is morally aordable having
the resources to prevent it.
Countries backing the IP waiver are not asking for charity, but for the right to develop and make their own vaccines, free
from the worry that they will be sued by patent holders.
The rapid development of several vaccines against COVID-19 is an unequalled scienc accomplishment, but the absence of
a system that secures equitable access to vaccines has uncovered deep inadequacies in the global governance systems for
health. We must crically examine our moral principles when it comes to vulnerable groups, pressing pharmaceucal com-
panies, normave agencies, and polical leaders to commit to an ethical behavior and pushing for iniaves that rst and
foremost promote ethical and equitable soluons.
Aording priority on the basis of economic or polical power is a clear deviaon from the public-health principles of maxim-
izing lives or life-years saved, and the commitment of assuring that lifesaving resources should not depend on naonality.
The United Naons (UN) Sustainable Development Goals (SDGs) instruct that universal preparedness for health requires a
radical systems approach: health must be seen in the broadest of contexts, with due aenon to social structures and infra-
structure, working and living condions and with strategies to counteract climate change, loss of biodiversity and human
destrucon of wild habitat.
A pandemic teaches that no one should be le behind and that no one is safe unl everyone is safe, and COVID-19 made
evident the consequences of not having health insurance or access to healthcare, not having water or a food supply during
Humanitarian News
W A B I P N E W S L E T T E R P A G E 15
lockdown situaons, or not having civil rights. However, the COVID-19 pandemic has shown the weak adherence of wealthy
naons to the commitments of that UN Agenda 2030, mainly the ‘leaving no one behind’. It has revealed democrac decits,
instuonal rigidity, weak accountability systems, and inadequate policy space that protects health-governance systems
from economic goals. We have seen how decient global accountability mechanisms are, and the consequences of leaving
health care at the mercy of its commercial determinants were clearly exhibited. The absence of legally binding mechanisms
that hold market actors accountable for failing to act for the public good and the consequences of this lack of proper regula-
ons were crudely exposed.
COVID epidemics has also shown that an ecient and independent supranaonal governance system is needed to take the
role of an eecve global coordinaon for medicines and vaccines be rapidly ready to be equitably delivered when an epi-
demic erupts.
The WHO is facing a crisis which is increasingly challenging the authority and presge of the United Naons' specialized
agencies in general and WHO in parcular. “Global health,” should really imply the consideraon of the health needs of the
people of the whole planet above the concerns of parcular naons. There are many concerns that the agency’s legimacy
and authority in global health maers have been undermined, showing that WHO priories are disproporonately inu-
enced by a few powerful donors. But the present mes require that supranaonal organizaons must be strengthened, not
undermined. A not minor issue is that realigning WHO’s nancial structure would likely safeguard both the agency’s autono-
my and member states’ trust, while alleviang concerns about undue inuence from powerful donors.
This crisis has taught that updated global governance mechanisms are needed that beer reect the contemporary geopo-
lical order and truly encourage internaonal collaboraon across sectors, through polical and legal soluons rooted in
commitments to jusce and shared global responsibility. The debate about the waiver of patents has brought wider debates
about pharmaceucal company power, predominance of geopolical strategy and lack of commitment to decrease the im-
pact of health inequalies. It is not simply the maer to become lost in the lights and shadows of a patent waiver. What
must remain clear is that the issues of jusce (equitable distribuon), benecence (helping other countries), and non-
malecence (avoiding harm to other countries) must be the priority of individuals and polical leaders.
This pandemic has been and it is sll being a dramac experience for any human being wherever and however they live. But
we cannot be fooled about it: we are not all in it together. COVID-19 is experienced unequally, with much more tragic conse-
quences for the most disadvantaged communies: it is not a socially neutral disease. We have seen as never before how the
impact of a disease is magnied by the pre-exisng social determinants of health, such as housing and work condions and
access to quality healthcare. We cannot aord adding to those long-term condions the deliberate restricons of the access
to the only current resource to decrease the disaster of COVID-19: the vaccinaon.
We are only risking our new shoes; we have only one morally acceptable choice: we must rescue the drowning child if we
want to rescue our own human dignity.
*The views expressed in this arcle are those of the author (Silvia Quadrelli) and do not necessarily reect the ocial posi-
ons of the Execuve Board or Internaonal Board of Regents of the WABIP.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 16
References:
1. Bozorgmehr K et al. Lancet. 2021 Apr 3;397(10281):1261-1262
2. Editorial: A patent waiver on COVID vaccines is right and fair. Nature. 2021 May; 593(7860):478
3. Ekström AM et al. Nat Med. 2021; 27, 739–740
4. Iacobucci G et al. BMJ 2021;373:n1182
5. Jecker NS et al. J Med Ethics. 2021;47:595-598
6. Nioi M et al. J Clin Med. 2020 Apr 16;9(4):1138
7. Rouw A et al. J Global COVID-19 vaccine access: a snapshot of inequality. hps://www.k.org/policy-watch/global-covid-19-
vaccine-access-snapshot-of-inequality/ Date accessed: December 10, 2021
8. Nioi M et al. Front Med (Lausanne). 2021 Nov 4;8:756623
Best Image Contest 2022 (1 of 3)
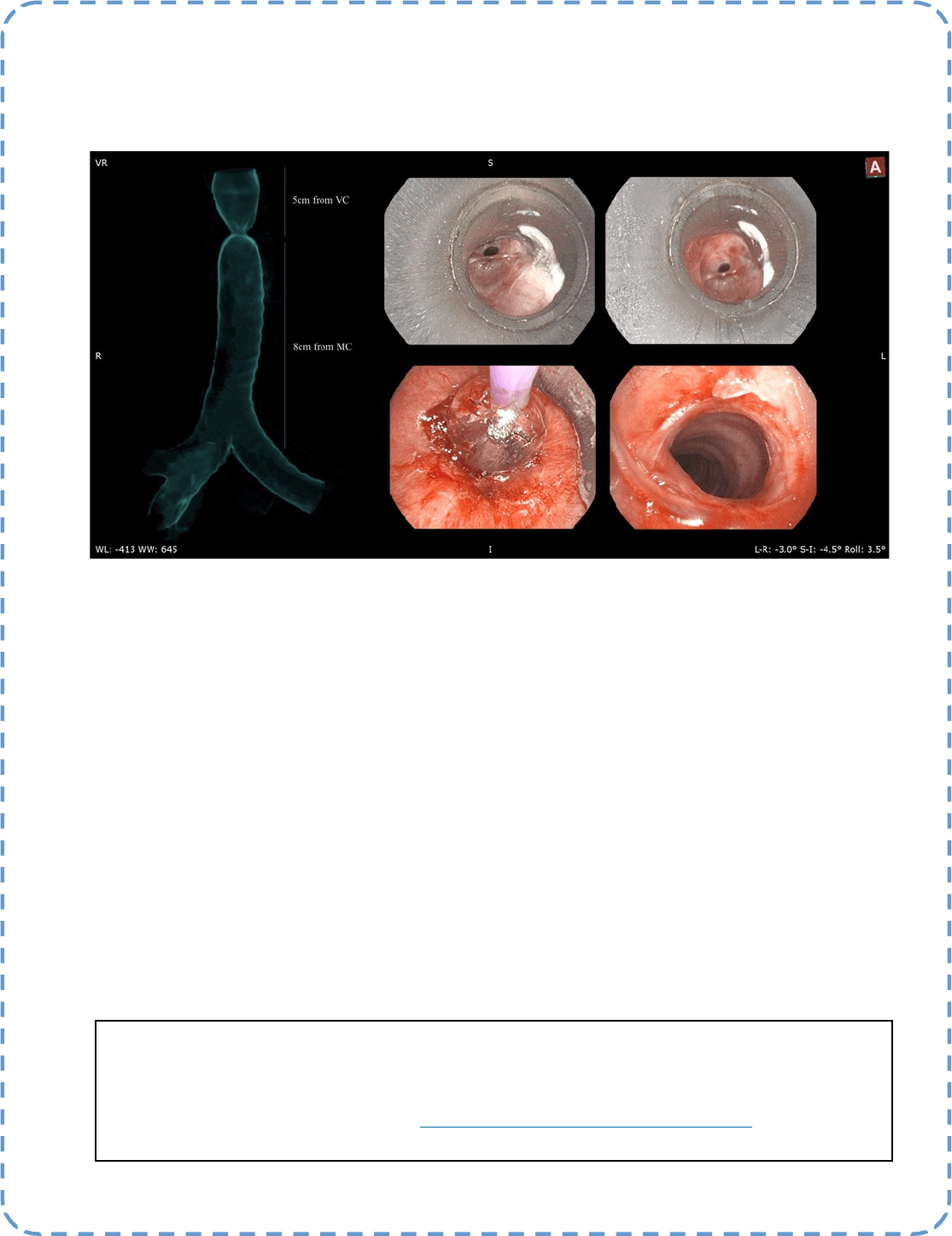
Descripon:
60 years old gentleman presented with insidious onset of stridor and exeronal dyspnea aer endotracheal
intubaon for a Killip-4 anterior myocardial infarcon a year ago. CT scan conrmed a ght stenosis at the
subgloc region which was successfully treated with balloon dilataon and mitomycin C applicaon via rigid
bronchoscope. Paent subsequently underwent denive surgical correcon successfully.
Submiers:
Dr. Kho Sze Shyang & Dr. Jamalul Azizi bin Abdul Rahaman
Best Image Contest
P A G E 17
This image is the 1 of 3 selected among 100+ submissions to our Best Image Contest held in late 2021. Please
stay tuned to the next Image Contest opening later this year. Find the above image and more at the WABIP
Academy Image Library at hps://www.WABIPacademy.com/imagelibrary
P A G E 18
WABIP News
Annual Board of Regents Meeng
This meeng shall be held on Saturday, March 12, 2022, and the Regents who represent their member society
will parcipate and vote on items mandated in our bylaws. The meeng is an integral part of compleng our an-
nual registraon to retain our status as a non-prot organizaon in Tokyo Japan.
WCBIP 2022 Marseille France
Marseille 2022 World Congress is coming this October in hybrid
format, and we could not be more excited to kick start our
oerings to WABIP members. We invite you to start the sub-
mission process for:
• Abstracts (Deadline May 2, 2022) Guidelines & submission
link at hps://www.wcbip.org/abstracts
• Video Fesval (Deadline July 1, 2022) Guidelines & submis-
sion form at hps://www.wcbip.org/videofesval
• WABIP Awards (Deadline July 1, 2022) Guidelines & submission forms at hps://www.wabip.com/
awards
Registraon for on-site and online parcipaon will be open in February 2022.
Endoscopic Ultrasound Secon – New members welcome
We are proud to announce that 190 members have joined this
new WABIP secon, and we are embarking on many related pro-
jects and acvies. We can sll accommodate a few new mem-
bers, and we welcome you to apply for Endoscopic Ultrasound
secon membership via hps://www.wabip.com/forms/
commiees
9th Asian Pacic Congress on Bronchology & Intervenonal Pulmonology
We would like to announce that the Asia-Pacic congress will now
take place in April 2023, moved from original October 2021 date. Dr.
Jamalul Azizi and his organizing commiee will will ensure an ex-
cing program with didacc lectures, case-based discussions, virtual
hands-on workshops, and more. Stay tuned to all related updates at
hp://www.apcb2021.com
What Are the Necessary Technologies and Techniques for Transbronchial Ablaon of
Pulmonary Nodules?
Ablaon techniques, including radiofrequency ablaon, microwave ablaon (MWA), and cryoablaon, are promising treatments for malig-
nant pulmonary nodules. Compared to percutaneous approaches, transbronchial ablaon therapy for pulmonary nodules has a more favourable
safety prole by virtue of avoiding pleural puncture (1-3), although the cumulave clinical experience remains limited. Challenges with transbron-
chial approaches include increased diculty accessing peripheral nodules and managing the ablaon margin, whereby potenal injury to the pleu-
ra and other major structures must be avoided.
A recent retrospecve study from Chan and colleagues (4) is informave and thought-provoking on successful transbronchial treatment of
pulmonary nodules. They summarized results from transbronchial MWA of 30 pulmonary nodules with electromagnec navigaon bronchoscopy
(ENB) guidance in a single instuon. Their procedure in a hybrid operang room included the following technologies: 1) cone-beam computed
tomography (CBCT) at baseline, aer posioning the catheter pre-MWA, and post-MWA, 2) ENB to navigate the MWA catheter to the target (±
uoroscopy), and 3) the Transbronchial Access Tool (TBAT) for accessing targets without a bronchus sign. Twenty-two nodules (73%) were in the
peripheral-third lung eld. Pneumothorax requiring chest tube inseron and hemoptysis occurred in 2 and 1 cases, respecvely. Transbronchial
MWA achieved local control over the follow-up period of median 12 months.
For pulmonary nodule ablaon, precise tool placement is essenal. ‘Navigaon’ and ‘conrmaon’ are separate components of precise
placement. Commercially-available navigaon modalies include virtual bronchoscopic navigaon, ENB, and augmented uoroscopy. They help
guide inseron of the bronchoscope and tools into the appropriate bronchus faster. However, selecng the correct bronchus does not mean the
tool p is opmally posioned. This disncon is important when deriving guidance from preprocedural CT images, as CT-to-body divergence
needs consideraon (5). Venlaon and instrumentaon can distort the regional parenchyma, resulng in a discrepancy between the expected
target locaon (i.e., based on preprocedural CT) and the actual target locaon just prior to ablaon. Consequently, the posion of navigated
Editor-in-Chief: Dr. Kazuhiro Yasufuku
Research
Primary Business Address:
Kazuhiro Yasufuku, Editor-in-Chief WABIP
Newsleer
c/o Judy McConnell
200 Elizabeth St, 9N-957
Toronto, ON M5G 2C4 Canada
E-mail: newsleer@wabip.com
P A G E 19
Associate editor:
Dr. Ali Musani
Associate editor:
Dr. Sepmiu Murgu
Tsukasa Ishiwata, MD, PhD
University Health Network
Kazuhiro Yasufuku MD, PhD
University Health Network
Alexander Gregor, MD
University Health Network
tools relave to the nodule must be conrmed by other modalies. Those oen used clinically include radial probe endobronchial ultra-
sound (RP-EBUS) and CBCT.
In the context of ablaon, CBCT has an advantage over RP-EBUS in that it can conrm catheter posion relave to the target and to
surrounding ssues, perming more precise calculaon of both the potenal ecacy and safety of the ablaon zone.
A major challenge with transbronchial ablaon, regardless the navigaon and conrmaon technologies used, is that target access
has convenonally depended on the presence of a feeding bronchus. Chan and colleagues overcame this issue by using TBAT. The TBAT (6),
and other plaorms like it (7), create alternave transbronchial routes to the target by tunnelling through the lung parenchyma from a pre-
selected bronchial puncture point. These techniques will be vital for successful ablaon of nodules without a bronchus sign, avoiding the
need for excessively large ablaon elds to fully encompass distant peribronchial targets.
To successfully and safely perform transbronchial ablaon of pulmonary nodules, several advanced technologies and techniques
are required. More studies are needed to condently conclude on the performance and safety of transbronchial ablave therapies. Moreo-
ver, the learning curve and cost-eecveness of combining such technologies have not been fully evaluated. Chan and colleagues have, how-
ever, established an important benchmark to guide future work.
References
1. Koizumi T et al. Case Rep Oncol Med. 2013;2013:515160.
2. Xie F et al. Respiraon. 2017;94(3):293-8.
3. Pritche M et al. CHEST. 2020;158:A1452-3.
4. Chan JWY et al. Transl Lung Cancer Res. 2021;10(4):1608-22.
5. Pritche MA et al. J Thorac Dis. 2020;12(4):1595-611.
6. Anciano C et al. J Bronchology Interv Pulmonol. 2017;24(3):253-6.
7. Sa S et al. Lung Cancer. 2018;124:125-9.
Research
P A G E 20
P A G E
21
WABIP ACADEMY- WEBCASTS
The WABIP has started a new educaon project recently: THE WABIP ACADEMY. The WABIP Academy will pro-
vide free online webcasts with new and hot topics that will interest pulmonologists and intervenonalists.
Current webcast topic: Tissue acquision for biomarker directed therapy of NSCLC
You can reach these webcasts by using this link: hp://www.wabipacademy.com/webcast/
www.bronchology.com Home of the Journal of Bronchology
www.bronchoscopy.org Internaonal educaonal website for
bronchoscopy training with u-tube and
facebook interfaces, numerous teachiing
videos, and step by step tesng and assess
ment tools
www.aabronchology.org American Associaon for Bronchology and I
ntervenonal Pulmonology (AABIP)
www.eabip.org European Associaon for Bronchology and
Intervenonal Pulmonology
W A B I P N E W S L E T T E R
Links
www.chestnet.org Intervenonal Chest/Diagnosc Procedures (IC/DP)
NetWork
www.thoracic.org American Thoracic Society
www.ctsnet.org The leading online resource of educaonal and
scienc research informaon for cardiothoracic
surgeons.
www.jrs.or.jp The Japanese Respirology Society
sites.google.com/site/asendoscopiarespiratoria/
Asociación Sudamericana de Endoscopía Respiratoria
P A G E 21