Volume 09
Issue 03
October 2021
Inside This Issue
Editorial, 2-3
Tips from the Experts, 4-6
Humanitarian News, 7-12
Best Image Contest, 13
WABIP News, 14
Research, 15
Links, 16
Lexical Considerations Regarding
Interventional Pulmonology: An Opinion
WABIP Newsletter
O C T O B E R 2 0 2 1 V O L U M E 9 , I S S U E 3
EXECUTIVE BOARD
Hideo Saka, MD
Japan, Chair
Stefano Gasparini,
MD
Italy, Vice-Chair
Silvia Quadrelli, MD
Argenna, Immediate
Past-Chair
David Fielding MD
Australia, Treasurer
Naofumi Shinagawa,
MD
Japan,
Secretary General
Philippe Astoul, MD
France, President
WCBIP 2022
Menaldi Rasmin, MD
Indonesia, President
WCBIP 2024
STAFF
Michael Mendoza
General Manager
Judy McConnell
Administrator
Kazuhiro Yasufuku
Newsleer Editor-in-
chief
P A G E 2
Stefano Gasparini
Polytechnic University of Marche Region
Department of Biomedic Sciences and Public
Health
Pulmonary Diseases Unit, Azienda Ospedaliero-
Universitaria “Ospedali Riuni”
Ancona, Italy
The denion “Intervenonal Pulmonology” was
ocially introduced in 2001 in a paper published by
Luis Seijo and Dan Sterman
1
. While in the paper the
term “Intervenonal Pulmonology” was limited to
dene “advanced bronchoscopic and pleuroscopic
techniques for the treatment of a spectrum of tho-
racic disorders”, such as rigid bronchoscopic
debulking and stenng, balloon dilataon, endo-
bronchial laser/cryo/electrocautery/brachitherapy,
in the immediately following years the meaning of
this denion has expanded. Today, we include in
the denion of Intervenonal Pulmonology all the
invasive or semi-invasive procedures performed by
pulmonologists not only for therapy but also for
diagnosis of respiratory diseases (bronchoscopy
and related techniques, thoracoscopy, thoracic
drainage inseron, percutaneous biopsies, pleural
biopsies, percutaneous tracheostomy). In a joint
ERS/ATS document
2
, Intervenonal Pulmonology
was dened as “the art and science of medicine as
related to the performance of diagnosc and inva-
sive therapeuc procedures that require addional
training and experse beyond that required in a
standard pulmonary medicine training pro-
gramme".
This term was immediately successful and has been widely
accepted by the Scienc Community. The most important
Scienc Sociees involved in the eld of thoracic endoscopy
changed their name and added “intervenonal pulmonolo-
gy”, like Word Associaon for Bronchology (WAB) which be-
came WABIP, European Associaon for Bronchology (now
EABIP), American Associaon for Bronchology (now AABIP).
Even the previous Journal of Bronchology, in 2009 became
Journal of Bronchology & Intervenonal Pulmonology
(JOBIP). In the last years several books tled “Intervenonal
Pulmonology”
3
were published, and in the chapters of these
books all the diagnosc and therapeuc techniques related
to bronchoscopy and thoracoscopy are included.
The main reasons for the success of this denion are three:
1) the previously used term of “thoracic endoscopy” is an
understatement since “endoscopy” means “to look in-
to” (from greek “endoscópesis”, a compound word consisng
of “éndon”, which means inside and “scopeín”, which means
to watch carefully). Today, most bronchoscopic/
thoracoscopic procedures involves some kind of maneuver or
sampling and are not limited to exploraon; 2) some pulmo-
nary intervenonal procedures are not based on endoscopy
(like drainage inseron, percutaneous biopsies); 3) the deni-
on “Intervenonal Pulmonology” underlines and emphasiz-
es the role of the pulmonologist as the professional gure
with the competences and the knowledges to perform such
procedures and reiterates that this eld of medicine belongs
to the pneumological specialty or to the Colleagues that are
involved in the diagnosis and treatment of respiratory diseas-
es.
Other speciales arrived before Pulmonology to understand
the importance of qualifying an area of their competence
with the term “intervenonal”. The dicon of “Intervenonal
Radiology” was coined in 1967 by Alexander Margulis
4
, Direc-
tor of Radiology Department at the University of San Francis-
co. A lile later is the birth of “Intervenonal Cardiology” by
Andreas Gruenzig from Zurich
5
, which in 1974 extended the
use of percutaneous angioplasty to coronary arteries, revolu-
onizing the therapy of ischemic heart disease.
If it is true that the term “Intervenonal” has been widely
accepted, it is equally true that there is some terminological
confusion, and frequently denions such as “intervenonal
bronchoscopy”, “intervenonal bronchology”, “operave
bronchoscopy”, “advanced bronchoscopy” are encountered.
W A B I P N E W S L E T T E R
P A G E 3
terminology used in Intervenonal Pulmonology will be
reached.
References
1) Seijo LM et al. N Engl J Med 2001; 344: 740-749
2) Bolliger CT et al. Eur Respir J 2002; 356-373
3) Principles and pracce of Intervenonal Pulmonology. A Ernst,
FJF Herth Eds. Springer Science, New York 2013
4) Margulis A. AJR 1967; 101: 265-286
5) Gruentzig A. Am Heart J 1982; 103: 779-783
6) Intervenonal bronchoscopy. Bolliger C et al. 2000
7) Hardavella G et al. Breathe 2015; 11: 202-212
8) Intervenonal Bronchoscopy. Mehta A, Jain P Eds. Springer Sci-
ence New York 2013
9) hps://www.cuimc.columbia.edu/pulmonary/clinical-centers/
intervenonal-bronchoscopy
What does it mean “Intervenonal bronchoscopy”?
In the book “Intervenonal Bronchoscopy” edited
by Chris Bolliger and Praveen Mathur
6
, interven-
onal bronchoscopy is dened as “all aspects of
diagnosc and therapeuc bronchoscopy, which go
beyond the techniques of inspecon, simple lavage
and biopsies of the tracheobronchial tree”. But, if
we look at some books, some papers and some
internet web sites, we nd that this denion is
somemes used to describe complex therapeucal
procedures (laser resecon, electrocautery, cryo-
therapy, stenng, photodynamic therapy)
7
, but at
other mes it includes also diagnosc procedures
(TBNA, EBUS-TBNA, electromagnec navigaon,
bronchoscopy in hemoptysis)
8
, and even BAL and
endobronchial biopsy
9
.
The term “intervenonal” in medicine, according to
the Cambridge Diconary, is “the act of interven-
ing, interfering or interceding with the aim of mod-
ifying the outcome”. According to this denion,
even a simple bronchoscopy aimed to verify the
condion of the airways may modify the diagnosis.
To introduce an instrument into the airways is al-
ways an intervenon. In other words, bronchosco-
py is a procedure that in any case belong to Inter-
venonal Pulmonology. The same concept can be
applied for the term “operave bronchoscopy”.
Concerning the term “advanced bronchoscopy”, it
could be confusing, since the burden between
basic and advanced bronchoscopy is blurred. What
today is an advanced technique, could become
basic in the future (TBNA was an advanced tech-
nique in the ‘80s, today it is considered basic; to-
day roboc bronchoscopy is an advanced tech-
nique, but maybe it could become roune and
basic in the future); furthermore, what is advanced
for somebody could be basic for others.
In conclusion, my opinion is that bronchoscopy is
always an operave and intervenonal procedure,
even when performed for simple diagnosc pur-
poses. I suggest to employ the denions of diag-
nosc and therapeuc bronchoscopy, both includ-
ed in the eld of “Intervenonal Pulmonology”.
Let’s leave the precious adjecve “intervenonal”
to our pulmonology specialty.
I hope that a discussion on this issue will take place
in our Associaon and that a standardizaon of the

Tips from the Experts
P A G E 4 V O L U M E 9 , I S S U E 3
Introducon
Recurrent respiratory papillomatosis (RRP) is a disease caused by infecon of the respiratory tract with human papilloma virus (HPV) sub-
types 6 and 11 [10]. RRP has an esmated incidence of 1.8 cases per 100,000 adults in the United States [2, 13]. Occasionally, papillomas
undergo malignant transformaon [1]. While vaccinaon could prevent development of RRP, once the papillomas develop, current standard
of care is removal via debridement or ablave therapy, most oen bronchoscopically when present in the trachea [1, 5, 11]. These means
include laser, argon plasma coagulaon, microdebrider, and photodynamic therapy [1]. Herein we outline the most common approaches to
bronchoscopic intervenon for RRP.
Indicaons, descripons, techniques, and complicaons for specic RRP intervenons
Indicaons for surgical management of tracheobronchial papillomatosis, in this case bronchoscopic intervenon, largely relate to maintain-
ing airway patency and/or palliaon of symptoms thought to be related to the presence of papillomas (e.g. stridor, wheezing, recurrent
pneumonia, and dyspnea) [1]. All modalies listed below are eecve at achieving this endpoint, albiet with diering technical aspects and
complicaons. Remission is unpredictable and re-intervenon is common [11].
Laser
There are several laser systems that have been used in the treatment of RRP, all allowing for applicaon of thermal energy which desiccate
and coagulate the ssues and minimize bleeding. Currently, carbon dioxide (CO2) laser is the preferred method of papilloma removal in the
otolaryngology pracces, however other lasers including neodymium:yrium aluminum garnet (Nd:YAG), potassium tanyl phosphate
(KTP), have also been used [5, 7, 15, 16] and oer similar characteriscs and rates of remission [1].
Technique for applicaon of laser includes use of a exible quartz ber advanced through a exible or rigid bronchoscope. Given the risk of
airway re, FiO
2
during laser operaon should be decreased to <0.4. Specialized ET tubes for laser have also been developed to minimize
complicaon of airway re should a exible bronchoscope be used. Care should be taken to maintain laser orientaon coaxial to the trache-
al lumen as laser penetraon into ssue can vary with dierent systems [7]. Other complicaons include airway perforaon and airway
stricture, incidence of which are thought to be lower with CO2 laser compared to other modalies [1].
Argon Plasma Coagulaon
Argon plasma coagulaon (APC) is an ablave therapy that uses a tungsten wire to deliver a spark to insuated argon gas which causes ioni-
zaon. The ionized gas creates an electrical arc to the nearest ground, in this case the ssue nearest the probe p. The plasma causes an
ablave, vaporizing, and coagulaon eect from the applied thermal energy. It has been used for the treatment of airway papillomas suc-
cessfully since 1997 [3].
Bronchoscopy Intervenons for Recurrent Respiratory Papillomatosis
Sepmiu Murgu, MD
The University of Chicago
Grady Hedstrom, MD
The University of Chicago

Tips from the Experts
P A G E 5 V O L U M E 9 , I S S U E 3
Technique includes introducon of a exible APC probe via a exible or rigid bronchoscope. Similar to laser, airway re is a concern at high
oxygen content, thus care should be taken to only apply APC at FiO2 <0.4. Separaon of the probe from the target ssue by a small distance,
<1cm, is necessary to achieve a plasma arc. Thus, APC should be considered a non-contact ablave therapy. Rare complicaons include air-
way burns and perforaon, and very rarely, gas embolism. Overall complicaons are thought to be rare (3.7%) [12].
Microdebrider
Microdebriders are considered an alternave to thermal energy techniques such as laser or APC. The device uses a rotatory cung cup at the
p of a rigid sucon catheter to facilitate rapid ssue removal [4]. Microdebriders have been compared with CO2 laser in prospecve manner
and found to be equally safe and eecve, with potenally lower procedural cost [8].
Technique includes introducon of the rigid microdebrider device via rigid bronchoscope as currently there is no exible opon. Sucon is
applied and contact with target papilloma facilitates cung and removal of ssue. Because ssue removal occurs without thermal energy,
there are no venlatory or FiO2 requirements for use and airway re is not a concern [4,8]. However, because ssue is cut and removed di-
rectly without thermal coagulave eects, bleeding is of concern, and it oen requires thermal energy for its control.
Photodynamic Therapy
Photodynamic therapy (PDT) is a technique that uses an infusion of a photosensizer, pormer sodium or Photofrin, prior to applicaon of
630 nm red light [6]. The photosensizer preferenally is retained in the papilloma cells and when acvated by red light, produces oxygen
free radicals leading to cytotoxic damage and death [10]. While most data published to date relate to its use in the larynx, a recent mulcen-
ter retrospecve case series outlined its use as safe and eecve for bronchoscopic use in tracheal lesions [6].
Technique includes infusion of pormer sodium, 2mg/kg, 48-72 hours prior to bronchoscopic intervenon [6]. A exible 630 nm red light
catheter is introduced via exible bronchoscopy near the target papilloma. The papilloma is then exposed to red light for several minutes.
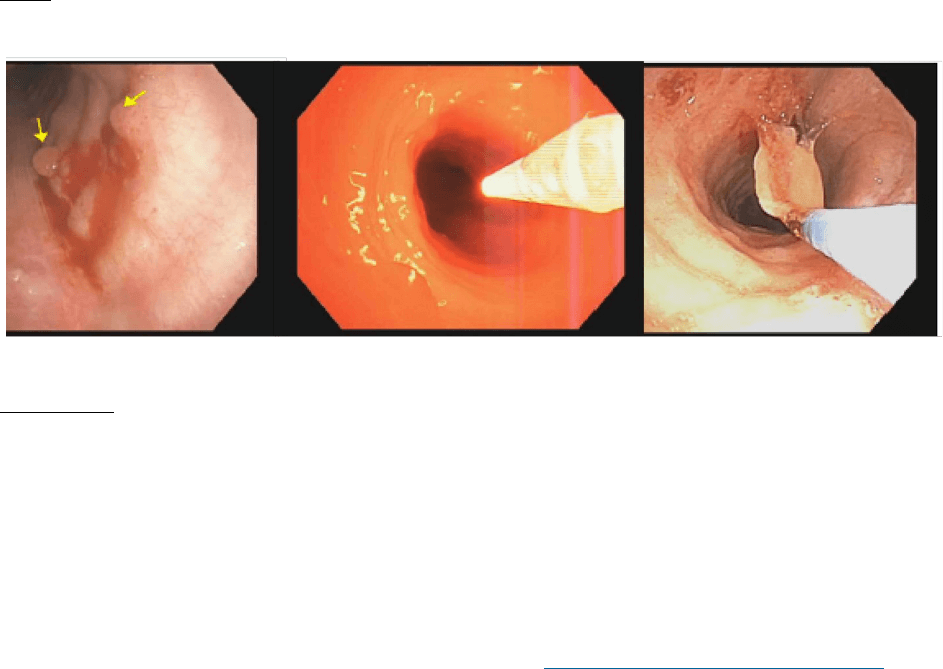
Cellular death results in sloughing of aected ssue over the following days to weeks (Figure). Repeat exible and/or rigid bronchoscopy for
debulking and cleaning of the aected area is necessary to prevent airway obstrucon from denuded ssue. Complicaons arising from PDT
are thought to be relavely rare, however include photosensivity reacons, airway obstrucon, airway perforaon, and potenally airway
stricture [6].
Other consideraons
HPV genomic DNA has been detected in the plume created by laser ablaon of papillomas [1]. Thus, it is recommended that for ablave ther-
apies, such as laser or APC, appropriate precauons and PPE be used by healthcare providers to reduce the risk of coinfecon. Apneic anes-
thesia and minimal use of jet venlaon may reduce airborne transmission.
Conclusions
There are several modalies for bronchoscopic intervenon which have been demonstrated to be safe and eecve for treatment of tracheal
or airway RRP. Selecon of technique should be individualized based on operator experience, local resources, and paent factors for minimiz-
ing potenal side eects. Repeat intervenon is very oen necessary and mulple approaches may be applied in a single paent.
Tips from the Experts
P A G E 6 V O L U M E 9 , I S S U E 3
Figure
Figure Legend
A cluster of lower tracheal papilloma lesions (le panel). Biopsies showed papilloma and transformaon to squamous cell carcinoma in situ.
PDT was performed with a 1 cm rigid ber, 200 J/cm, adjacent placement (middle panel). At 48 hours post light applicaon, there was airway
edema with minimal sloughing of necroc material, removed using forceps (right panel).
References :
1. Alkotob M et al. J. Bronchol. Interv. Pulmonol. vol. 11, no. 2, Apr. 2004, pp. 132–139.
2. Armstrong L et al. AOHNS, vol. 125, no. 7, 1999, p. 743., hps://doi.org/10.1001/archotol.125.7.743.
3. Bergler W et al. J Laryngol Otol. vol. 111, no. 4, 1997, pp. 381–384., hps://doi.org/10.1017/s0022215100137387.
4. Casal R et al. Respirology, vol. 18, no. 6, 2013, pp. 1011–1015., hps://doi.org/10.1111/resp.12087.
5. Derkay C et al. The Laryngoscope, vol. 118, no. 7, 2008, pp. 1236–1247., hps://doi.org/10.1097/mlg.0b013e31816a7135.
6. Glisinski K et al. Photodiagnosis Photodyn Ther. vol. 30, 2020, p. 101711., hps://doi.org/10.1016/j.pdpdt.2020.101711.
7. Khemasuwan DJ. Thorac. Dis, vol. 7, no. Supplement 4, Dec. 2015, pp. S380–8., hps://doi.org/10.3978/j.issn.2072-1439.2015.12.55.
8. Pasquale K et al. The Laryngoscope, vol. 113, no. 1, 2003, pp. 139–143., hps://doi.org/10.1097/00005537-200301000-00026.
9. Patel N et al. Rhinology & Laryngology, vol. 112, no. 1, 2003, pp. 7–10., hps://doi.org/10.1177/000348940311200102.
10. Proo AE et al. Photodynamic Therapy: Mechanisms, 1989, hps://doi.org/10.1117/12.978012.
11. “Recurrent Respiratory Papillomatosis or Laryngeal Papillomatosis.” Naonal Instute of Deafness and Other Communicaon Disorders, U.S. Depart-
ment of Health and Human Services, hps://www.nidcd.nih.gov/health/recurrent-respiratory-papillomatosis.
12. Reichle G et al. Pneumologie, vol. 54, no. 11, 2000, pp. 508–516., hps://doi.org/10.1055/s-2000-8254.
13. RRPF.org, hp://www.rrpf.org/about.html.
14. Venkatesan N et al. Otolaryngol. Clin. North Am, vol. 45, no. 3, 2012, pp. 671–694., hps://doi.org/10.1016/j.otc.2012.03.006.
15. Zeitels S et al. Curr Opin Otolaryngol Head Neck Surg, vol. 15, no. 6, 2007, pp. 394–400., hps://doi.org/10.1097/moo.0b013e3282f1b2.
16. Zeitels S et al. Ann. Otol. Rhinol. Laryngol. vol. 115, no. 9, 2006, pp. 679–685., hps://doi.org/10.1177/000348940611500905
Humanitarian News
W A B I P N E W S L E T T E R P A G E 7
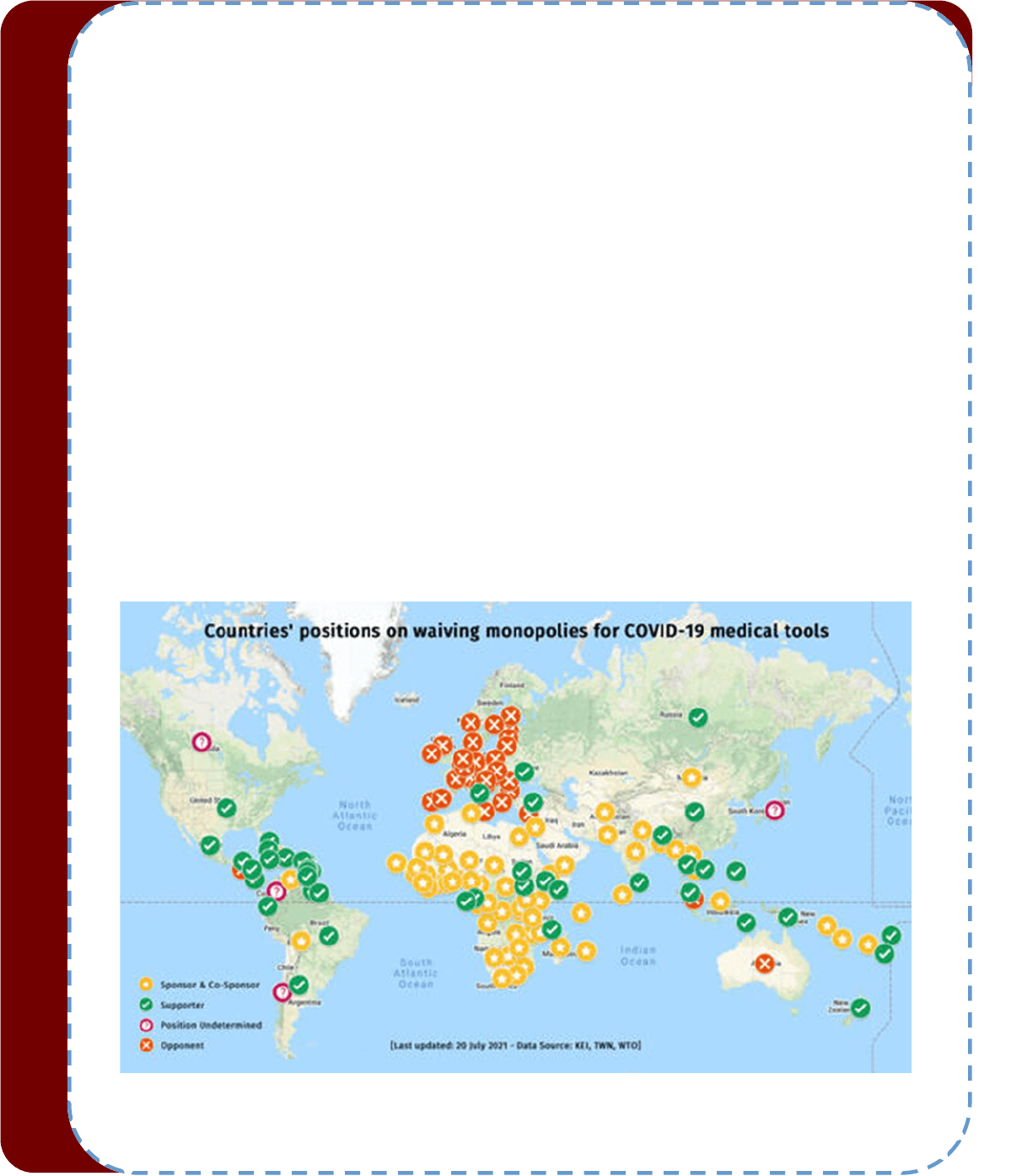
The COVID-19 Vaccine Patent Waiver: An Acon to Advance
Equitable Access to Medicines?
“Health is a fundamental human right indispensable for the exercise of other human rights. Every human being is entled to
the enjoyment of the highest aainable standard of health conducive to living a life in dignity.”
Commiee on Economic, Social and Cultural Rights - General comment No. 14 on the highest aainable standard of health
As specied in the General comment no. 14, the right to health is an inclusive right. It extends not only to mely and appro-
priate health care but also to the underlying determinants of health, such as: access to safe and potable water and adequate
sanitaon; an adequate supply of safe food, nutrion and housing; healthy occupaonal and environmental condions; and
access to health-related educaon and informaon.
Health equity relates to the fairness in distribuon of health resources and outcomes. This applies both to equity between
cizens in specic countries as well as between countries. There is general consensus amongst scholars, polical bodies,
opinion leaders and general populaon that solving these inequies—the huge and remediable dierences in health be-
tween and within countries—is a maer of social jusce, essenal for the linked concepts of fairness, jusce, and freedom.
However, much before the beginning of the COVID-19 epidemic, it was obvious that at a naonal and global level, that ob-
jecve of increasing equality could not be further from reality. Historically, ethical principles in health policy have oen been
disregarded for vulnerable groups, with the distribuon of life-saving drugs considered too expensive and unsustainable and
the recipients deemed unt and unworthy. The Alma Ata Declaraon could not expose it more clearly “The exisng gross
inequality in the health status of the people, parcularly between developed and developing countries as well as within coun-
tries, is polically, socially, and economically unacceptable and is, therefore, of common concern to all countries”. But more
than 40 years later lile real acon has been taken.
The problem is not new, but in Anthony Fauci’s words, the pandemic “shone a bright light on our own society's failings”. Dur-
ing this pandemic, unacceptable disparies intra and inter-countries have achieved their highest levels in the modern era
and have highlighted the serious adverse eects of using an unfeered market-orientated approach to health development.
The ethical distribuon of life-saving medical and public health intervenons amongst vulnerable groups has rarely been
respected. Factors as esmang how much lives are worth linked to an individual's country of origin, the pharmaceucal
industry's priorisaon of prot, the manipulaon of vulnerable groups in clinical trials made the human right to health un-
aainable for many people. The COVID-19 pandemic was an opportunity to remediate that long-standing history of unethical
pracces in global health by making a safe, eecve vaccine accessible to all iniang a new era of global health more ori-
ented to ethical decision making.
At the beginning of the pandemic, vaccine companies such as Pzer stated that they would make sure low-income countries
“have the same access [to the vaccine] as the rest of the world.” Yet what we are seeing today is a massive global disparity in
the allocaon of available vaccines.
High-income countries, represenng just 20% of the global adult populaon, have purchased more than half of all vaccine
doses, resulng in huge disparies of available doses. Of the remaining doses, 33% have been purchased by low-middle in-
come countries (LMIC), who account for 81% of the global adult populaon; and 13% have been by COVAX. Wealthy coun-
tries such as the U.S., Canada, UK and others formalized bilateral agreements with the companies producing the vaccines in
order to their assure their posion at the front of the line well before the vaccines were available. Those strategies to secure
preferenal access, may be understandable within the naonal context, but clearly jeopardise supplies for other countries.
As an example, the COVAX iniave was established to assure and equitable distribuon of vaccines but its goal was never
achieved as vaccine naonalism shown by countries' decisions to accumulate vaccines and inoculate groups that are not at

Humanitarian News
W A B I P N E W S L E T T E R P A G E 8
high risk (as teenagers) has substanally reduced the availability of vaccines. It is esmated that most of low-incomes coun-
tries will not be vaccinated unl the last month of 2023.
It may be argued that If the pharmaceucal companies pung in years of research and development are based in and sup-
ported by high-income countries, those countries have a right to receive their products rst, but having vaccines to cover
low risk populaon when most countries don’t even have enough vaccines to protect their health care workers or their el-
derly populaons seems dicult to jusfy from an ethical point of view. Beyond the global interest of reducing variants, the
moral imperave to provide a fair distribuon of vaccines cannot be ignored.
These deals do not only talk about naons or regions priorising their cizens. Most of all, these negoaons remark the
power of patent-holders. That power allow large pharmaceucal companies to make decisions of high public impact about
access to vital lifesaving healthcare, and at what price.
Patents are generally seen as necessary incenves for the development of medicines. However, the COVID epidemic has
brought to light many quesons that need be asked around the extent of that control in the hands of private patent-holders.
For example, it is known that the research and development by pharmaceucal companies is largely supported by govern-
ment subsidies, which makes the price cited for most medical products mulple mes the real producon cost. Considering
that subsidies given by governments to pharmaceucal companies are nanced with the taxes paid for by cizens (including
vulnerable groups), this unreasonable pricing of drugs and vaccines is of dubious morality and denies vulnerable groups their
right to health. In fact price pracce turn most pharmaceucal rms into the most protable companies compared to other
industries.
The World Trade Organizaon’s Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) has clearly stat-
ed that while eorts to protect the intellectual property rights of innovang companies has encouraged investment in drug
discovery, the creaon of the 20-year patent for new drugs has meant that many poor people all over the world have not
been able to aord them. This unfairness was patently evident during the 1990s when life-saving anretroviral drugs were
inially denied to those in developing countries because of the unreasonably high costs of the drugs. Patent-holders can
even refuse licenses to third pares to produce a patented medicine transforming the patent-holder in the only provider of
that medicine resulng in dangerous limitaons for its supply. It also impact the price of a medicine as patent-holders can
charge high prices for licenses or access.
In order to decrease the unfairness of distribuon between rich and poor countries, many organizaons, academic leaders
and even policy makers have urged to take concrete acons. Amongst the possible soluons is a vaccine patent waiver,
which was proposed by India and South Africa back in October of 2020. This would allow other companies, including those in
developing countries, to make generic brands of exisng vaccines. The intellectual property temporary waiver proposal
would allow countries to choose not to apply or implement patents and other exclusivies that could obstruct the produc-
on and supply of COVID-19 medical tools, unl global herd immunity is reached. Aer the inial proposal of India and South
Africa in October 2020, now the proposal is ocially endorsed by 58 sponsoring governments, and 100 countries supporng
the proposal overall.
However a small number of wealthy countries, as the U.S. , the European Union, UK, Japan, and Australia amongst others,
opposed the proposal. In a remarkable decision, on May 5th, United States President Biden decided to change U.S. policy,
backing the proposal.
Maintaining patents is ethically unacceptable as it means deliberately refusing to help countries in desperate need and vio-
lates the principle of benecence (doing good for others), jusce and non-malecence (not creang harm for others) and it
results in concrete consequences as the occurrence of evitable deaths. This is because vaccine patents, which are a form of
intellectual property (IP) rights, lead to create monopolies that contribute to increased prices and decreased access. This
injusce has been described as ‘vaccine apartheid’ because it creates obscene disparies in vaccine access.
Under internaonal trade law, mechanisms exist for States to issue compulsory patent licenses – following certain criteria
and in specic circumstances. Compulsory licenses allow the State to grant permission to a third party to produce the pa-
tented invenon, e.g. medicine, without the patent-holders consent.
Waiving patents is not a radical or new proposal and it would not be the rst me that patent waivers were allowed. In
2001, the “Doha Declaraon on TRIPS and Public Health” eliminated patents on drugs for HIV, allowing for cheaper produc-
Humanitarian News
W A B I P N E W S L E T T E R P A G E 9
on and more aordable products. It was also the case during the 1980’s with the hepas B vaccines. However tradional-
ly, countries have been reluctant to use compulsory licenses because of the strong industry opposion. But in the devas-
tang context of Covid-19 many social actors are urging for change. Some countries have adopted legal measures to facili-
tate compulsory licensing where needed for Covid-19 and other States should follow soon. However, in general, compulsory
licensing is not complete and mely enough for COVID-19 vaccines: it is a slow mechanism as it requires separate negoa-
ons between countries and companies, and mainly because would not provide access to key elements in producon such
as trade secrets, it maintains barriers for collaboraon and import and export of products and materials and does not cover
future vaccines. The waiver would remove any obstacles for global vaccine producon, present and future. However, in the
light of the opposion, it seems that without a strong internaonal movement and direct pressure, that sort of acon is un-
likely.
Under the 1995 Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS), pharmaceucal companies have
at least 20 years from ling a patent to prot from their investments in developing pharmaceucal products throughout the
world. Global IP rights, whether adopted in accordance with TRIPS, or subsequent bilateral and mullateral agreements, are
part of a wider legal system which facilitates that powerful actors such as the European Union (EU) and the USA have includ-
ed TRIPS-plus clauses that oen force countries of the Global South to concede to more stringent patent protecons in order
to gain trade advantages and also to escape trade sancons. In so doing, IP law commodies medicines that are essenal to
human survival and well-being, and sacrices the lives and health of the poor and vulnerable in order to priorize corporate
protability. That comes from the common interpretaon by the internaonal IP system that healthcare products and ser-
vices derive their value from their tradability and not from their nature of public goods.
The World Trade Organizaon (WTO) Doha Declaraon on TRIPS and Public Health recognizes human rights and allows
states to use all of the ‘exibilies’ within the TRIPS regime to protect public health, agreeing on the need for access to med-
icines in a public health emergency. However, this internaonal consensus on employing TRIPS exibilies of IP has always
been strongly contested by pharmaceucal companies and their host governments and even during this pandemic the
aempts of LMIC to try to obtain a TRIPS waiver to increase their supply of vaccines have been unsuccessful.
Crics of a waiver argue that this process would not create rapid increase in supply, because the complex manufacturing
processes and the length of me it takes to build new factories are amongst the major obstacles to increasing the global sup-
ply of vaccines and so, patents are not the liming factor. It is also said that compeon for access to the raw materials
could slow the already working producon and even results in decrease of supply. And of course they claim that if compa-
nies have no prot incenve to create these new health care products, then we may see a drop in the investments of the
pharmaceucal rms. This later seems a more than quesonable argument taking into account the magnitude of billionaire
prots of the pharmaceucal companies. Moderna's share price has gained more than 700% since February 2020, while
BioNTech has surged 600% and CanSino Biologics' stock is up about 440% over the same period. For example it is expected
Moderna to make $13.2 billion in Covid-19 vaccine revenue in 2021. It must be kept in mind that vaccine producon was
possible because the company has received billions of dollars in funding from the US government for development of its
vaccine. It means that in most of the cases, the nancial risk of developing the vaccines was eecvely carried by the taxpay-
ers, funded by public money which makes at least somewhat dubious that they are only property of these companies and
could be freely used to deliver these enormous prots.
Voluntary licensing is oered as an alternave. However, arrangements where patent-holders voluntarily license their pa-
tents freely on reasonable terms are needed. Precedents cauons not to let our hopes run too high about those voluntary
contribuons. As Yuanqiong Hu, Senior Legal and Policy Advisor at MSF’s (Médecins sans Froners) Access Campaign said.
“Governments that oppose the monopoly waiver proposal know that simply asking pharmaceucal corporaons to voluntari-
ly do the right thing will not get us anywhere, when these aempts have so far failed to secure global access to COVID-19
medical tools for people who urgently need them. It’s me for change, not charity”.
Potenal opons to patent waiver could be to increase direct patent licensing, allowing the rms producing vaccines to part-
ner with specic companies to increase producon while sll protecng their intellectual property. Addionally, exporng
exisng vaccines could alleviate the shortage of vaccines in some countries. At May 2021, the U.S. had donated only around
1% of the vaccines it has produced although President Biden has recently pledged to donate 20 million U.S.-made vaccines.
On the other hand, many middle-income countries like China and Russia or low-income countries like India have already ex-
ported a signicant proporon of their vaccines to other countries.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 10
Vaccine donaons are not the soluon to the scarcity of COVID-19 vaccines in many countries. Yet, the potenal number of
surplus vaccine doses purchased by wealthy naons are suciently large to help with near-term vaccine demands while in-
vestments are made in technology transfer to LMICs and in scaling up global manufacturing capacity for vaccines. Maximiz-
ing the potenal of vaccine donaons in this pandemic depends on vaccine doses going where they can do the most good,
but there is no full agreement where they should go. COVAX has been cricized for its populaon-based allocaon scheme
that does not direct most of its early vaccine supplies to the sengs at the greatest risk of otherwise having high COVID-19
death rates. But even if Covax in the most opmisc scenario, succeeds in reaching its targets, only 20% of people in low and
middle income countries (LMICs) will be fully vaccinated by the end of 2021, because those planned targets were very mod-
est based on a “scarcity mindset”—expecng that total global doses would be limited and rich naons would likely hoard the
supply. But the rapid development of several vaccines allowed the rich naons to buy more doses than they could ever use
and are not sharing with anyone. Canada has procured enough doses to vaccinate all its cizens 10 mes over. UK could vac-
cinate everyone in the UK eight mes over.
On the other hand, naons donang COVID-19 vaccines bilaterally have used their donaons (as any internaonal bilateral
cooperaon) more as a means of polical inuence than advancing global vaccine equity and saving lives. It is imperave
that donor countries keep the commitment of grounding future COVID-19 vaccine donaons in epidemiology and not geo-
polics.
But even when donaons are the quickest way to increase availability of vaccines they are not enough. Donaons are a char-
ity model and aer the ‘‘gi’’ is over the vaccine supply dilemma remains. It is imperave to create a sustainable model for
LMICs to be able to make their own vaccines to ensure populaon-wide vaccinaon soon enough to prevent thousands of
deaths. The model of donaons rather than allowing for equitable vaccine access as a basic human right for all people every-
where, turned to a charitable donaon and market purchase scheme through the COVAX iniave. This type of model,
which focuses on charity and not rights, keeps the colonial ideology’, in parcular by addressing the untold idea that to be
colonized was to be inferior. Vaccine access should not be a queson of charity but of states fullling their human rights
commitments under internaonal law.
A waiver of intellectual property protecons on covid-19 vaccines, including on their components and raw materials is an
urgent rst step that must be taken soon. It will need to be reinforced by transfer of technical knowledge from vaccine mak-
ers in the global north to regional hubs or directly to manufacturers in the global south and by the nancial help needed for
wide subsidizaon of manufacturing in LMICs.
The People’s Vaccine Alliance, a grouping of several non-prot, non-governmental organizaons including Global Jusce
Now, Oxfam and Amnesty Internaonal, is calling for the pharmaceucal rms to share their technology so that global pro-
ducon of vaccines can be quickly increased, claiming that the scarcity of vaccines is arcially created by these monopolies,
and that there is enough space for these companies to make a more than decent return instead of obscene prots that cre-
ate a few new billionaires. Addionally Dr Christos Christou, MSF Internaonal President has claimed that “Countries must
stop obstrucng and show the leadership required to deliver on the ‘global solidarity’ they have so oen declared during this
pandemic”. “It’s me to champion access to medical tools for everyone, wherever they live.”
Internaonal human rights law provides a universal framework for advancing global health with jusce, transforming moral
imperaves into legal entlements. The right to the highest aainable standard of health, rst arculated in 1946 in the
WHO Constuon, has evolved through the progression of treaes such as the Internaonal Covenant on Economic, Social
and Cultural Rights (ICESCR). Nearly every country in the world has now raed at least one internaonal agreement that
imposes specic obligaons that lead to the realisaon of the right to health, including explicit obligaons to prevent, treat
and control epidemics.
The United Naons (UN) Commiee responsible for interpreng the ICESCR, has emphasized that states ‘have a duty to pre-
vent intellectual property and patent legal regimes from undermining the enjoyment of economic, social and cultural rights’,
and that the IP regime should be interpreted and implemented in a manner supporve of the duty of states ‘to protect public
health’.
Arguments to defend IPRs simply do not hold. The protecons of IPRs to the vaccine companies are causing health and soci-
oeconomic suering globally, rather than alleviang them. Delaying vaccine access for billions of people threatens the con-
nuaon of the pandemic and development of new dangerous variants.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 11
The inequalies and injusce concerning access to vaccines and medical supplies needed during COVID pandemic do not
occur out of the blue. The commodicaon of essenal medicines is the consequence of the prevalent system of global capi-
talism that allows manufacturers and states to value nancial prot over human life. The worsening of inequality crisis trig-
gered by COVID-19 is framed by the economic model and has meant an increase in poverty, unemployment and a colossal
suering for millions of people while, at the same me, allowed some of the world’s largest corporaons to get billions of
dollars in prots to shareholders then increasing the gap between rich and poor in an unprecedented magnitude. COVID-19
should be the opportunity for radically restructuring business models (at least in health care) with the purpose of granng a
decent status of wellbeing for everyone by creang an economy for all. It is necessary to keep in mind that we are able to
live together because all the members of the society (having raonalized it or not) have signed the basic covenant, the social
pact, to come together and form a people, a collecvity. That is the foundaon of democracy, the collecve renunciaon of
the individual rights and freedom that each one would have in the State of Nature, in order to design authories directed to
the get the good of all considered together. That social contract includes the idea of reciprocated dues: the authority is
commied to the good of the individuals who constute it, and each individual is likewise commied to the good of the
whole. That social pact requires the collecve percepon that each individual is really geng from the authority the preser-
vaon of their wealth, the protecon of their lives, liberty, and well-being in general, Locke easily imagine the condions
under which the contract with the government or the economic and polical elites is destroyed, driving men feel jused in
resisng the authority. It has been well said “Let no man pull you so low as to hate him” but the imperave of our me is
“Let no man pull him so low as to hate you”.
The me for declaraons and pompous words is over. It is urgent to act and prevent suering and death for thousands and
thousands of people. And it will not be done without understanding that the pandemic is not over unl it's over everywhere.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 12
References
1. Goncalves G. BMJ 2021;373:n1249
2. Kohler JC et al. BMC Med 18, 193 (2020). hps://doi.org/10.1186/s12916-020-01661-3
3. McMahon A. Journal of Medical Ethics 2021;47:142-148.
4. Médecins Sans Fronères. Countries obstrucng COVID-19 patent waiver must allow negoaon hps://www.msf.org/countries
obstrucng-covid-19-patent-waiver-must-allow-negoaons Date accessed: August 1, 2021
5. Rouw A et al. Global COVID-19 vaccine access: a snapshot of inequality. hps://www.k.org/policy-watch/global-covid-19-vaccine-
access-snapshot-of-inequality/ Date accessed: July 14, 2021
6. Sekalala S et al. BMJ Global Health 2021;6:e006169.
7. United Naons Human Rights Oce of the High Commissioner (OHCHR). Internaonal covenant on economic, social and cultural
rights, 1966. Available: hps://www.ohchr.org/documents/professionalinterest/cescr.pdf
8. Wilkinson RG et al. (2003). Social Determinants of Health: The Solid Facts. Geneva: World Health Organizaon.
*The views expressed in this arcle are those of the author (Silvia Quadrelli) and do not necessarily reect the ocial posi-
ons of the Execuve Board or Internaonal Board of Regents of the WABIP.
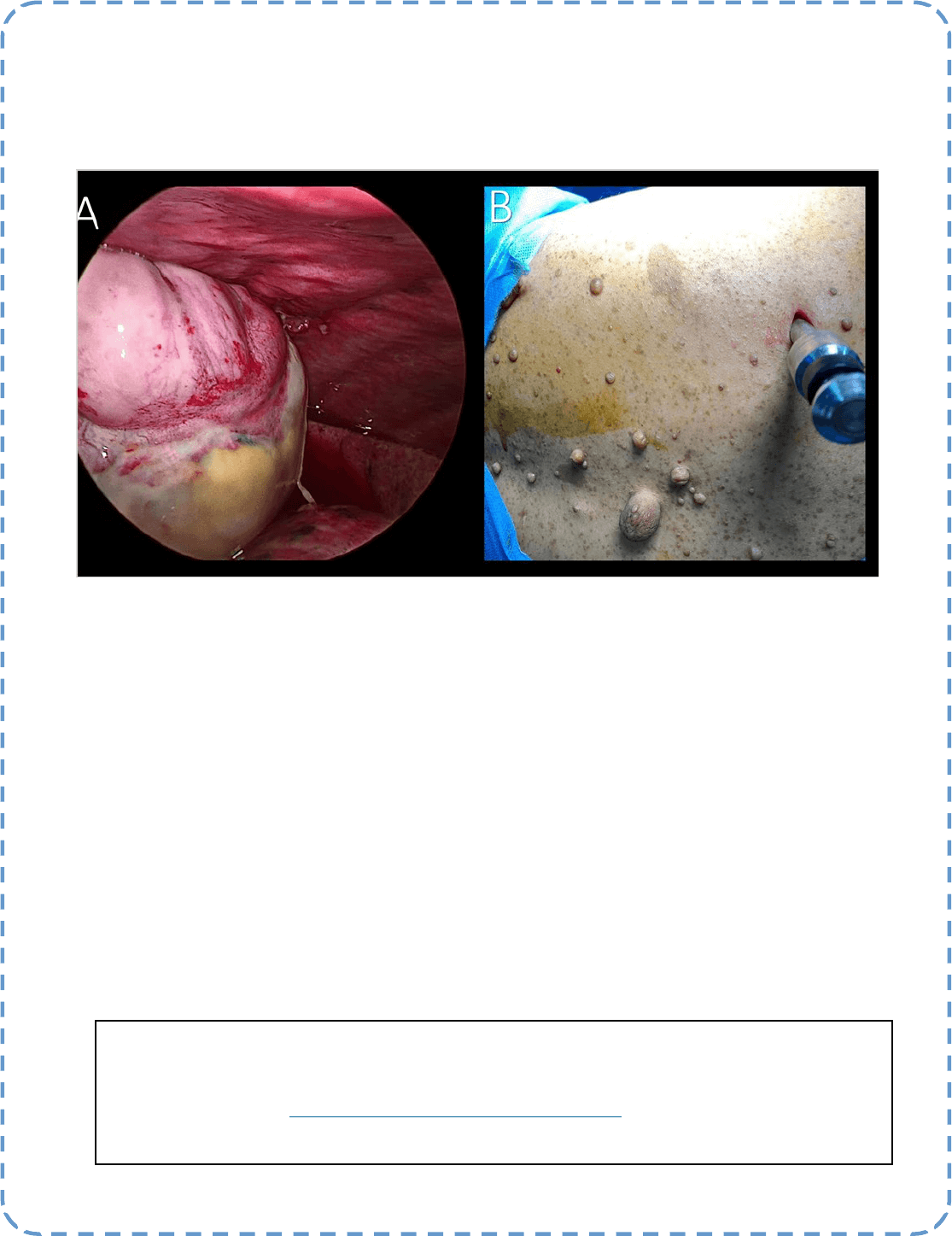
Best Image Contest 2021 (3 of 3)
Descripon:
Malignant Peripheral Nerve Sheath Tumor involving the pleura (A) in paent with Neurobromatosis (B)
Submiers:
Dr. Syeda Samia rasheed, Dr. Varun, Dr. Tiyagesh, Dr. Hari Kishan Gonuguntla
[Division of Intervenonal Pulmonology, Yashoda Hospitals, Hyderabad, India]
Best Image Contest
P A G E 13
This image is the 1 of 3 selected among 100+ submissions to our Best Image Contest held in late 2020. Please
stay tuned to the next Image Contest opening later this year! Find the above image and more at the WABIP
Academy Image Library at hps://www.WABIPacademy.com/imagelibrary

P A G E 14
WABIP News
New EBUS-TBNA Secon
Thank you to all those who applied for this new WABIP secon. We are happy to
announce 110 people joined from over 30 countries. Furthermore, we are
pleased to welcome Dr. Atul Mehta, Dr. Rocco Trisolini & Dr. Takahiro Nakajima
as secon coordinators. Under the auspices of these three, the secon will em-
bark on many new projects and acvies that improve WABIP members’
knowledge and technical skills of EBUS-TBNA. Please visit the secon page at
hps://www.wabip.com/ebus for all the latest news & updates from the sec-
on.
Invitaon to WCBIP 2022 Marseille, France
We would like to cordially invite you to join us in MARSEILLE, France, for
the 22nd WCBIP/WCBE from October 6th to 9th, 2022.
Organized by the WABIP and IBES, our biennial internaonal meeng is
dedicated to Bronchology and Intervenonal Pulmonology and will oer
high-caliber scienc programs with emphasis on new bronchoscopy
techniques, technologies and hands-on procedure workshops in which
you can meet and collaborate with colleagues from all around the world.
The pandemic has changed the format of conferences in general. And as
we have seen in our most recent WCBIP, purely virtual events can be just
as successful as tradional ones. The 22nd WCBIP shall be a “hybrid” event that will adopt this new format of meengs while
accommodang those who can be on-site in beauful Marseille, France.
In this congress, we will reinforce the importance of intervenonal pulmonology in this ever-changing world. Indeed globalizaon
marks a break in physical space and a break in communicaon mes that permeate our daily lives and medical pracces. We will
maximize communicaon technologies to oer equal educaon regardless of aendees’ places of parcipaon. This presents a
great opportunity for our 10,000 worldwide WABIP members to get all the latest informaon regarding advances in technologies,
educaon, and research in the eld of lung airway and pleural disorders through our numerous didacc lectures, interacve ses-
sions, and expert panel discussions.
We warmly welcome you in Marseille in October 2022 for this excing event to share scienc experse, but also to meet friends
and enjoy the gentle and sincere hospitality of the people by the Mediterranean Sea. Visit the congress site at hps://
www.WCBIP.org
Navigaon Bronchoscopy Webinar 2021
We are pleased to announce our Navigaon Bronchoscopy course is now being
oered as a Zoom webinar and for FREE to all WABIP members. Under the direcon
of Dr. Erik van der Heijden and team, this 2-day webinar will cover:
• The idencaon of paents suitable for navigaon bronchoscopy
• The design of clinical work-up that should enable a navigaon bronchoscopy program
• Disnguishing the dierent navigaon guidance techniques, pro’s and con’s
• Performance of dierent navigaon bronchoscopy techniques
• Interpretaon of navigaon technique results and drawing conclusions
Registraon starts in early November 2021. Please visit hps://www.wabip.com/navigaon for more informaon.
New secon coordinators:
Dr. Atul Mehta, Dr. Rocco Trisolini, Dr. Takahiro Nakajima
Hideo Saka, MD (Chair WABIP), Philippe Astoul, MD, PhD (President WCBIP),
Hervé Dutau, MD (President WCBE)
Don’t Listen To The Person Who Has The Answers, Listen To The Person Who Has The Quesons! (Albert Einstein)
Lung cancer staging is paramount in determining the therapeuc approach, especially surgery vs. no surgery. Nodal staging is one of the crical
components of staging and perhaps the most controversial one due to the sampling of the precise locaons or lack thereof.
The current guidelines from the American College of Chest Physicians for mediasnal staging for peripheral clinical stage IA tumor (negave nodal
involvement by CT and PET) suggest that invasive pre-operave evaluaon of the mediasnal nodes is not required (Grade 2B).
Nonetheless, studies have shown that CT and PET negave nodes can be posive with invasive sampling such as Endobronchial Ultrasound-guided
Transbronchial Needle Aspiraon (EBUS-TBNA) in upwards of 10% of the paents with peripheral T1 disease. Other studies have concluded that N2
and N3 disease is seen in up to 11-13% of the paents with T1 lesions.
One must wonder why such high nodal posivity in the ipsilateral and contralateral nodes with small peripheral lesions. One of the possible con-
founding factors might be the “denion” of peripheral vs. central lesions. Dierent authors have used dierent denions of peripheral, including
distance from the pleura, distance from the mediasnum, medial and lateral thirds, etc. The queson one must ask is, considering similar growing
data, is it safe to not perform invasive staging of the mediasnum in paents with T1 peripheral lesions or to revisit the current staging strategy?
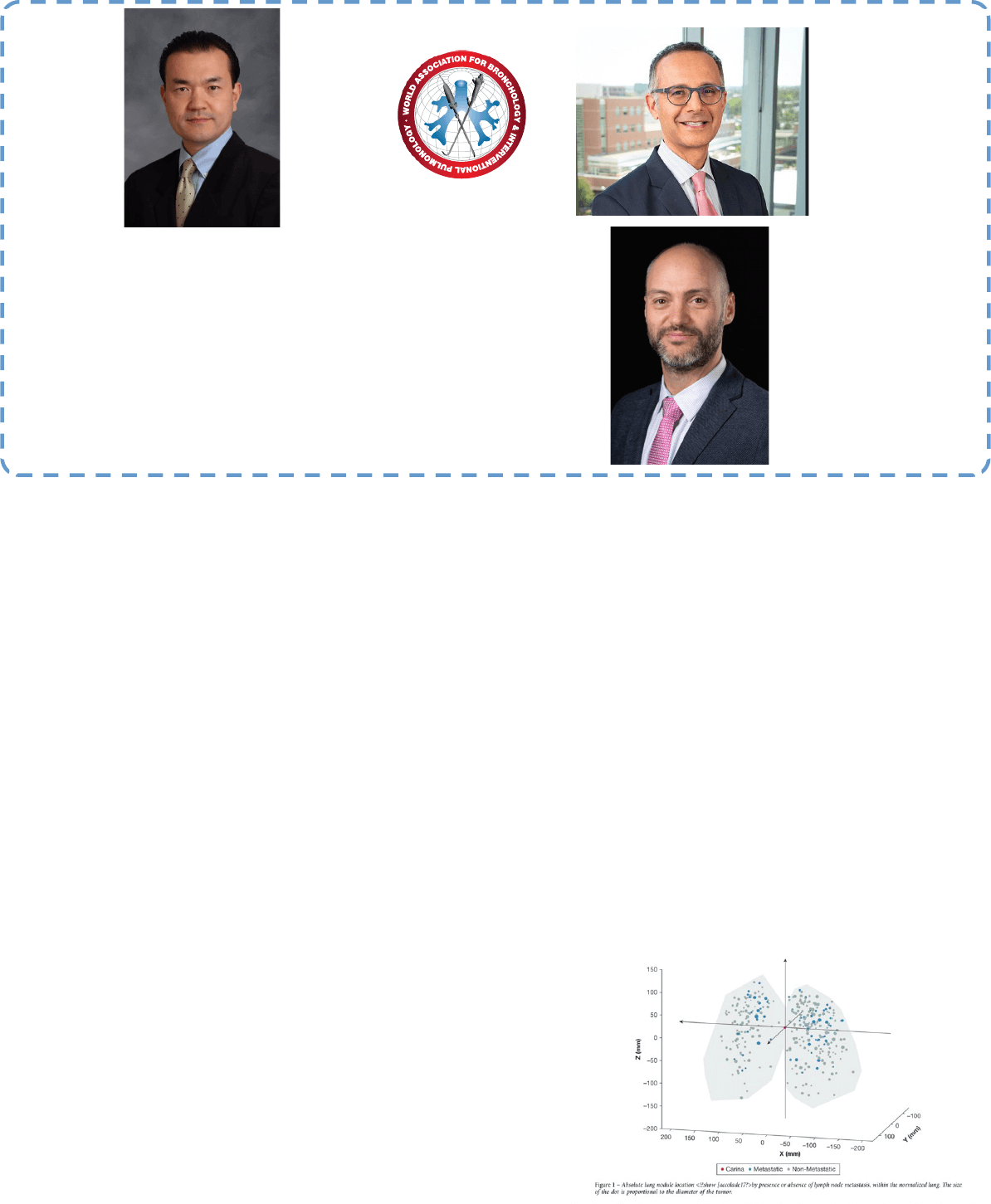
A recent study by DuComb et al. published in May 2020 CHEST (1) looked at the prevalence of N2/N3 diseases in the radiologically occult medias-
num with T1 tumors (cT1N0M0) in non-small cell cancer (NSCLC). The authors used the Naonal Lung Screening Trial data. They used X, Y, and Z
coordinates (Fig 1) from the main carina to evaluate the centrality of the nodule. This is a relavely novel and objecve technique. They found no
associaon between nodule locaon (central or peripheral) and the risk of nodal involvement. They also did not nd any dierence in nodal in-
volvement based on tumor size (within T1) or locaon. The authors found approximately 8% radiologically occult mediasnal involvement on EBUS
TBNA or another invasive sampling of the mediasnum and hilum. Hence, they recommend expanding the invasive staging to all peripheral T1 lung
tumors regardless of their centrality, size, or locaon. Some potenal limitaons of
the study include 1, lack of systemac use of PET scans in staging in this study pop-
ulaon, which has shown increased sensivity over CT for mediasnal nodal in-
volvement 2, lack of standard denion of central and peripheral in the previous
studies liming fare comparison to the this study’s data 3, lack of proven dierence
in the management and outcomes with single staon radiologically occult N2 dis-
ease.
I believe there is enough growing evidence to quesons the current algorithm of
staging strategies and perform more studies like Dr. DuComb’s to move the needle
on the precise therapy for lung cancer.
Reference: DuComb et al; CHEST 2020; 158(5):2192-2199
Ali I. Musani MD
Editor-in-Chief: Dr. Kazuhiro Yasufuku
Research
Primary Business Address:
Kazuhiro Yasufuku, Editor-in-Chief
WABIP Newsleer
c/o Judy McConnell
200 Elizabeth St, 9N-957
Toronto, ON M5G 2C4 Canada
E-mail: newsleer@wabip.com
P A G E 15
Associate editor:
Dr. Ali Musani
Associate editor:
Dr. Sepmiu Murgu
Figure 1: Reprinted from “Chest, 2020 Nov;158(5):2192-2199., DuComb EA,
Tonelli BA, Tuo Y, Cole BF, Mori V, Bates JHT, Washko GR, San José Estépar R,
Kinsey CM., Evidence for Expanding Invasive Mediasnal Staging for Peripheral
T1 Lung Tumors”, with permission from Elsevier.
P A G E
16
WABIP ACADEMY- WEBCASTS
The WABIP has started a new educaon project recently: THE WABIP ACADEMY. The WABIP Academy will pro-
vide free online webcasts with new and hot topics that will interest pulmonologists and intervenonalists.
Current webcast topic: Tissue acquision for biomarker directed therapy of NSCLC
You can reach these webcasts by using this link: hp://www.wabipacademy.com/webcast/
www.bronchology.com Home of the Journal of Bronchology
www.bronchoscopy.org Internaonal educaonal website for
bronchoscopy training with u-tube and
facebook interfaces, numerous teachiing
videos, and step by step tesng and assess
ment tools
www.aabronchology.org American Associaon for Bronchology and I
ntervenonal Pulmonology (AABIP)
www.eabip.org European Associaon for Bronchology and
Intervenonal Pulmonology
W A B I P N E W S L E T T E R
Links
www.chestnet.org Intervenonal Chest/Diagnosc Procedures (IC/DP)
NetWork
www.thoracic.org American Thoracic Society
www.ctsnet.org The leading online resource of educaonal and
scienc research informaon for cardiothoracic
surgeons.
www.jrs.or.jp The Japanese Respirology Society
sites.google.com/site/asendoscopiarespiratoria/
Asociación Sudamericana de Endoscopía Respiratoria
P A G E 16