Volume 09
Issue 01
January 2021
Inside This Issue
Editorial, 2
Technology Corner, 3-6
Tips from the Experts, 7-9
Humanitarian News, 10-15
Best Image Contest, 16
WABIP News, 17
Research, 18
Links, 19
Editorial: 21st WCBIP 2020 at a Glance
WABIP Newsletter
J A N U A R Y 2 0 2 1 V O L U M E 9 , I S S U E 1
EXECUTIVE BOARD
Hideo Saka, MD
Japan, Chair
Stefano Gasparini,
MD
Italy, Vice-Chair
Silvia Quadrelli, MD
Argenna, Immediate
Past-Chair
David Fielding MD
Australia, Treasurer
Naofumi Shinagawa,
MD
Japan,
Secretary General
Philippe Astoul, MD
France, President
WCBIP 2022
Menaldi Rasmin, MD
Indonesia, President
WCBIP 2024
STAFF
Michael Mendoza
General Manager
Judy McConnell
Administrator
Kazuhiro Yasufuku
Newsleer Editor-in-
chief
P A G E 2
Guangfa Wang MD
Beijing, China
President WCBIP 2020
We are pleased to report that the 21st congress
and the rst virtual congress of the WABIP was an
astounding success. This 2 ½ day event was com-
prised of world class presentaons by IP experts
from North America, South America, Europe, Africa,
Oceania and Asia.
In the evening of Nov 19, 2020 (Beijing me), the
opening ceremony began with a brief introducon
video on history of intervenonal pulmonology, to
its phenomenal growth, and to the current state of
the WABIP with nearly 10,000 members worldwide.
The ceremony also highlighted the rapid develop-
ment of IP in China. Myself, the president of WCBIP
2020, underscored the complexies organizing this
event, especially during the age of COVID-19. Also
in the ceremony were leaders from Chinese Thorac-
ic Society, Chinese Endoscopist Associaon, Chi-
nese Medical Associaon and China Naonal
Health Commission. They expressed their sincerest
gratude and warm congratulaon on the con-
gress, and especially to our colleagues ghng
against COVID-19. Last but not least, WABIP Chair
Prof. Silvia Quadrelli gave a wonderful presentaon
on the WABIP, and announced the WABIP Awards
recognizing those with signicant contribuons to
bronchology and intervenonal pulmonology.
The total number of registrants is 13,240 from 72
countries and regions, and the total visits to the
congress is 162,177. The most viewed session was
“Intervenonal pulmonology in the pandemic of
COVID-19”, which had 32,613 total viewers. And
ed for 2nd most popular sessions were “the Chal-
lenges of COVID-19 pandemic to Intervenonal
Pulmonologists” by myself and “Clinical Ulity of
Ultrathin Bronchoscopes” by Dr. Masahide Oki
from Japan.
While COVID-19 was indeed a hot topic of the con-
gress, lung cancer remained one of the main focus-
es of the event. Many topics and discussions were
related to early diagnosis, precision staging, genec
or pathologic technologies and intervenonal therapies.
Early lung cancer therapies with PDT, microwave, radiofre-
quency or cryotherapy aroused great interest from the audi-
ences. These novel technologies might be the standard ther-
apies to lung cancer tomorrow. Addionally, the interven-
onal therapies aracted great aenon to the aendees
either on dierent modalies, complicaons, long term out-
comes and peri-procedure care. Stem cell and gene therapy
on COPD were also discussed on the congress. The congress
also covered other technologies or elds in bronchology and
intervenonal pulmonology such as benign or malignant air-
way stenosis, cryobiopsy, thoracoscopy, trans-vascular or
trans thoracic modalies and IP educaon. Suce to say,
WCBIP 2020 oered a full spectrum of topics on bronchology
and intervenonal pulmonology.
Lastly, we are pleased to have had a closing ceremony
aracng thousands of audiences globally. The ceremony
began with “Forbearance with Bronchoscopy A Review of
Gratuitous Indicaons”, a presentaon by Dr. Atul Mehta,
which highlighted the boundary of bronchoscopy procedures
and reminded us these technologies should be not be used
for gratuitous indicaons. Addionally, organizing commiee
member Dr. Jie Zhang announced 5 best oral winners and 10
best poster winners for their excellent presentaons based
on the scoring of session chairs. I gave a summary of the con-
gress, emphasizing parcipaon of 256 conrmed speakers
who conducted 398 speeches in 125 academic sessions. Only
3 speakers were absent from the congress. Among 50 oral
presentaons, only four were absent.
Also in the closing ceremony, the new chair of WABIP, Dr.
Hideo Saka, had armed the success of the congress and
expressed his gratude to all involved. He also noted some
improvement in the future WCBIPs. Last but not least, as per
tradion in all WCBIP closing ceremonies, the WABIP ag was
transferred (but virtually this me) to Dr. Philippe Astoul who
will be organizing the next WCBIP in 2022 in Marseille,
France.
In conclusion, the congress created a milestone for WABIP
with the above menoned number of parcipants, sessions,
and over 25 company sponsors, and 17 industry symposia
and workshops. But there is no mistaking that we owe the
success of this congress to you and WABIP members who
submied over 600 abstracts and parcipated in our many
oerings. It has been my honor and pleasure to be the 21st
President of the WCBIP. Let us take sasfacon in the suc-
cess of WCBIP 2020, while we look forward to WCBIP Mar-
seille and having another wonderful scienc event .

Technology Corner
Currently Available EBUS-TBNA Needles
INTRODUCTION
The oncological approach to lung cancer was revoluonized forever aer the introducon of linear EBUS in the early 21st century
[1,2] as a tool for invasive mediasnal staging. The development and improvement of the materials and equipment used are ongo-
ing and are unlikely to end soon - something that should always be in the mind of those who deal with cases as complex and chal-
lenging as lung cancer can be. Therefore, since Olympus launched their rst EBUS-TBNA needle, the dedicated 22-gauge TBNA nee-
dle (NA-201SX-4022, Olympus, Tokyo, Japan)[3]; several other needles have emerged on the market. The purpose is to achieve the
most reliable sample, less trauma to the biopsied ssue, increased safety for the paent and the life of the bronchoscope and im-
proved ergonomics for the bronchoscopist. In addion, other diagnoses are also possible using EBUS, such as sarcoidosis, lympho-
ma and granulomatous infecous diseases - situaons in which the maintenance of adequate ssue architecture is even more im-
portant.
In this arcle, we will review the current needles available on the market and their parcularies.
BACKGROUND
Important qualies for EBUS-TBNA needle:
• Ergonomics: ergonomic handle for comfortable use by bronchoscopy.
• Safety: easy and safe locking mechanism, avoiding accidental protrusion of the needle during puncture and needle passage.
• Elegance and soness: needle penetraon as smoothly as possible, so the force necessary to cross the airway and the lymph
node capsule is minimized, avoiding damage to the carlage and contaminaon of the sample with airway material and blood.
• Flexibility: adequate exibility to reduce the distance from the p of the bronchoscope with the airway wall that occurs when
it is inserted into the distal poron of the working channel.
• Visibility: Echogenic p for adequate real-me visibility of the needle under ultrasound during the procedure.
In order to encompass all these characteriscs in the best possible way, several needles have emerged on the market over the
years as new technologies have been developed and new needs have been perceived.
W A B I P N E W S L E T T E R
P A G E 3
Kazuhiro Yasufuku MD, PhD, FRCSC
Division of Thoracic Surgery,
Toronto General Hospital,
University Health Network
Camila Greggianin MD
Division of Thoracic Surgery,
Toronto General Hospital,
University Health Network

CLINICAL APPLICATION - CURRENT NEEDLES AVAILABLE ON THE MARKET [4–9]
There is no published clinical trial comparing the accuracy of all available needles, so the current ones will be listed, highlighng their par-
cularies and potenal advantages. In this arcle, we will not cover mini-forceps.
Olympus
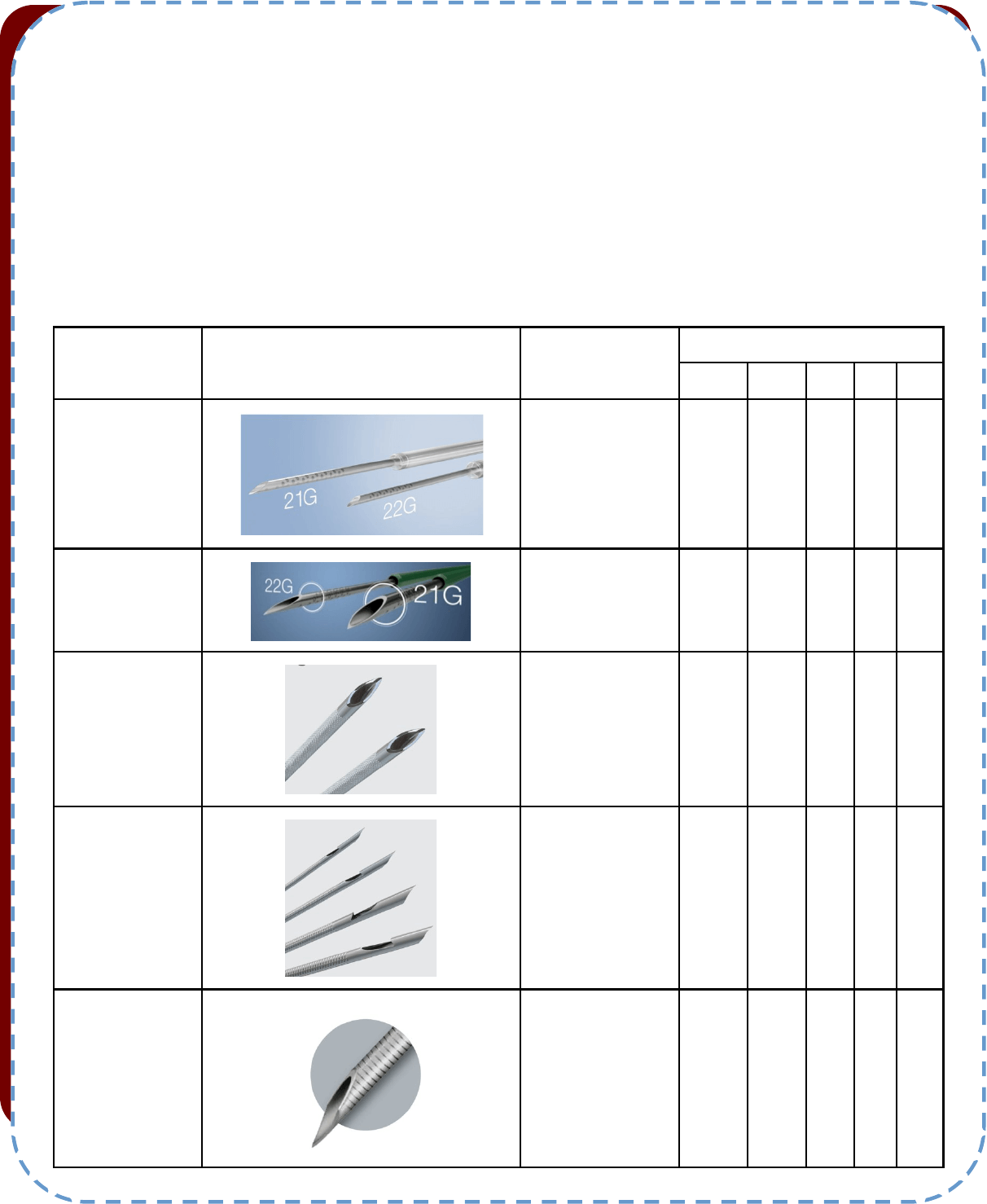
• ViziShot:
The classic needle developed since its prototype together with the EBUS linear bronchoscope. The available sizes are 21g and 22g.
• ViziShot 2:
The design and the material of the outer sheath have been revised which now provides beer exibility of the needle with 10 degrees
more angulaon when set on the bronchoscope. The p of the sheath is also green in color, which allows for easier endoscopic viewing.
There is also less movement of the outer sheath when advancing the needle out. The p of the needle is redesigned to be sharper, for a
less traumac ssue inseron. The available sizes are 25g, 22g, 21g.
Within the Vizishot 2 family, there is also the 19g FLEX needle, which, due to its internal diameter of 1 mm, is able to sample ssue for his-
topathological analysis, not only cytological. Despite the larger diameter, due to the spiral laser cuts along the sides of the needle surface,
the exibility is improved compared to the classical ViziShot lineup. The result is a greater angle which facilitates the visualizaon of the
most challenging lymph node staons.
Recently, the newest 25g size Vizishot 2 needle was launched. This needle can cover all the quality expected for the product, with extreme
smoothness during penetraon. In general, smaller needles generate less trauma in the sample, and therefore less blood contaminaon -
which is a crucial factor during rapid on-site cytological evaluaon.
Cook Medical
• EchoTip
R
Ultra
In its design, this needle features a highly exible spiral sheath, with the aim to facilitate access to regions where greater bronchoscope
angulaons are required. In addion, the p is a ball p type conguraon. Available in sizes 22g and 25g.
• EchoTip ProCore
R
This Cook needle is designed for the acquision of histological material, regardless of caliber, due to the design of its p. The 22g needle is
designed with a built-in ball p, while the 25g needle has a beveled p. Both, although dierent, aim to incise lymph node ssue during the
passage of the needle and collect the material inside the needle.
Boston Scienc
• Expect
TM
Pulmonary
Available in sizes 22g and 25g, the material of this needle is cobalt-chromium which is 24% harder than stainless steel (data provided by the
company), thus being more resistant to deformaon aer several passages and excellent tracon properes. However, due to the rigidity
of the needle the inseron angle of the needle is not as steep as the Olympus needle. It also has great clarity in the echographic image. A
non-inferiority was shown in a study comparing 22g with 25g needles[10].
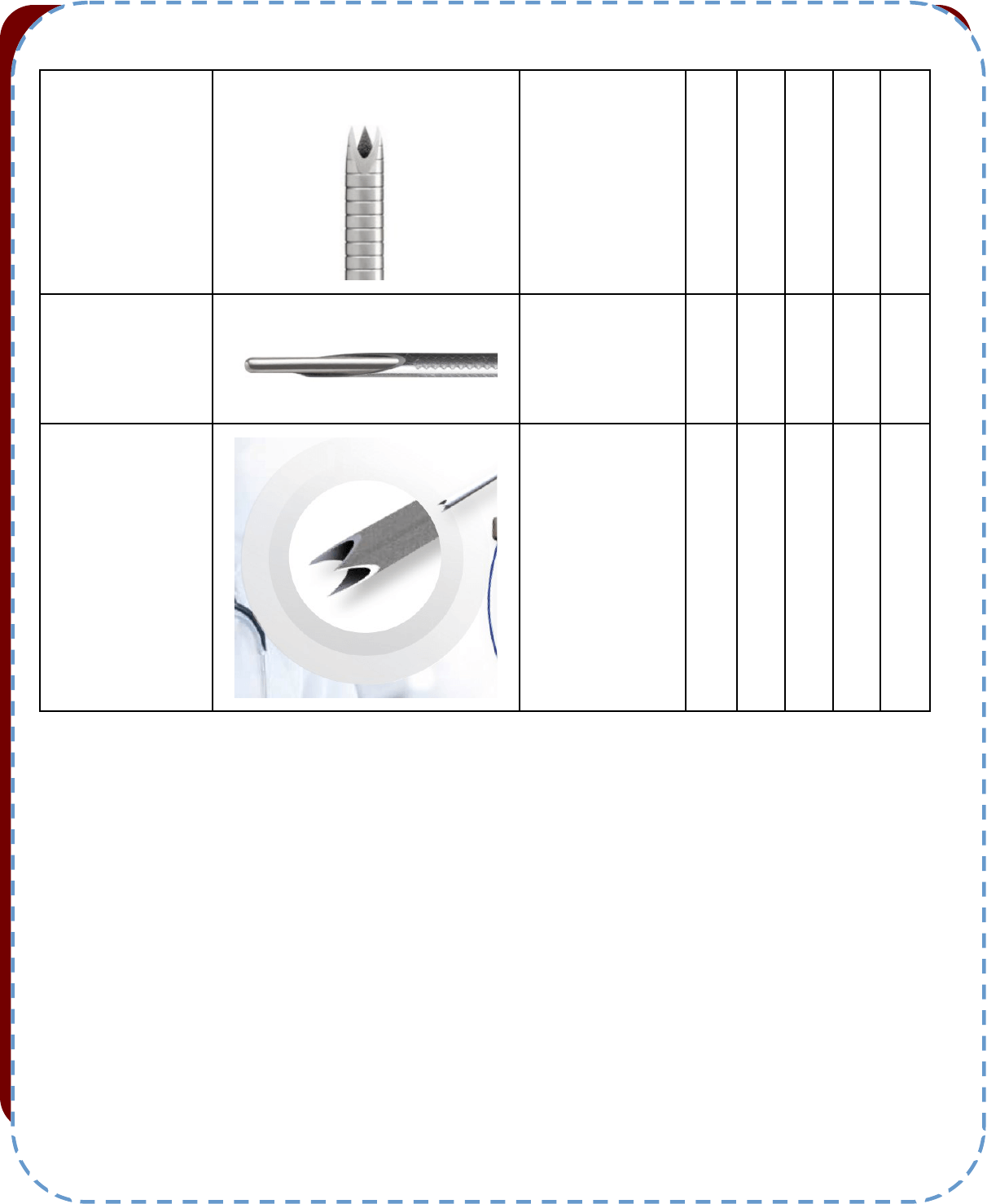
• Acquire
TM
Pulmonary
The main feature of this needle is its Franseen style p. This design was already used for other radiological approaches to ne-needle punc-
ture and aims to collect histological material even for smaller diameter needles. Like the Expect, it is also made of chromium-cobalt, main-
taining its same qualies: good needle penetraon, beer ability to push, resistance to torsion and deformaon aer several passes. How-
ever, similar to the Expect needle, the inseron angle of the needle is not as steep as the Olympus needle.
W A B I P N E W S L E T T E R P A G E 4
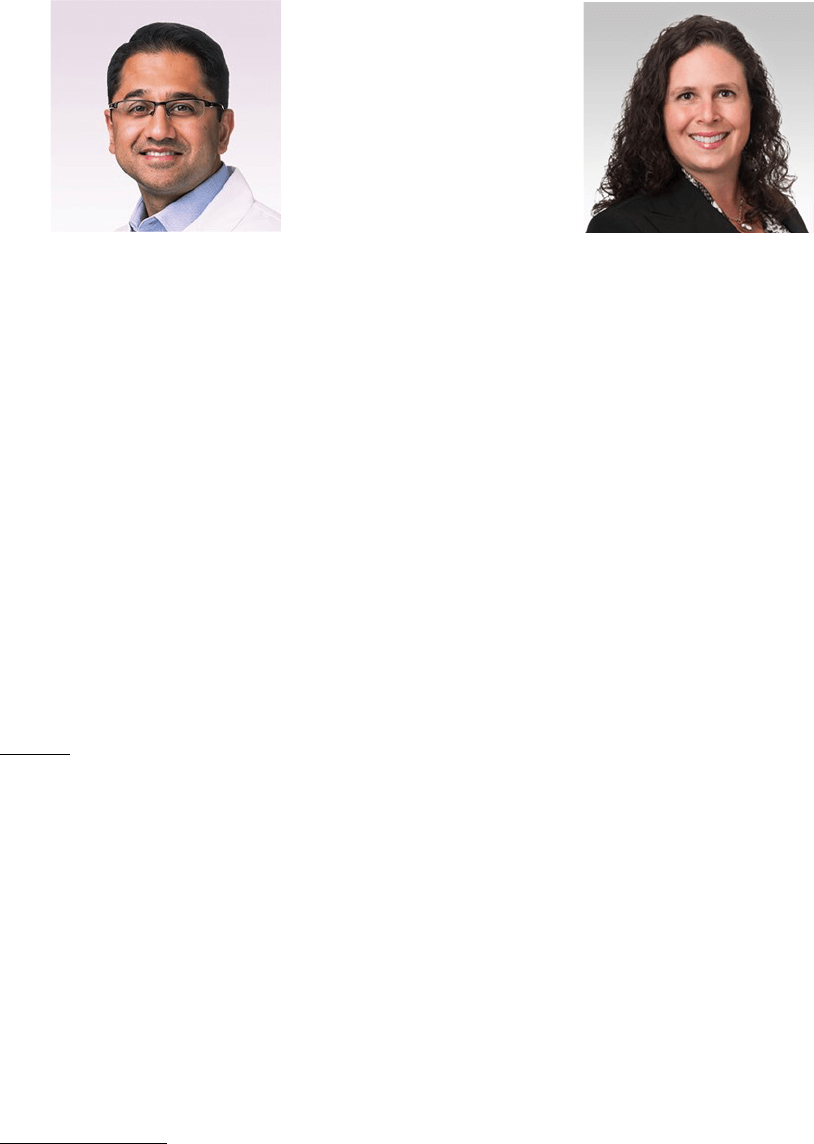
Medi-Globe
• SonoTip® EBUS Pro Flex:
Derived from the EUS needles already made by the company. It is the rst needle completely made from Ninol. Made of ninol or stain-
less steel, compable with Olympus, Pentax and Fujilm EBUS-scopes. Sharpe p as most of the other needles. Available only in size 22g.
• SonoTip TopGain® EBUS-TBNB:
It has a p like Boston Acquire, which is called a "crown cut" by the manufacturer, with the aim of reducing the fragmentaon of the mate-
rial when the needle is introduced. Available only in size 22g, but in stainless steel and ninol.
Table 1: Comparison between needles.
W A B I P N E W S L E T T E R P A G E 5
Brand and type of
the needle
Picture
EBUS scope com-
patibility
Needle size (g)
25 22 21 20 19
Olympus
ViziShot
Olympus
x x
Olympus
ViziShot 2
Olympus x x x
x
Cook Medical
EchoTip® Ultra
Olympus, Pentax x x
Cook Medical
EchoTip Pro-
Core®
Olympus, Pentax x x
Boston
Scientific
Expect
TM
Pulmonary
Olympus x x
CONCLUSION
Minimally invasive strategies with the greatest possible accuracy should be the focus of today's bronchoscopist. Performing a trans-
bronchial puncture is not limited to the bronchoscopic technique alone. The acquision of an adequate sample for diagnosis starts with the
indicaon of the procedure, adequate training, knowledge and choice of the needle according to the diagnosc hypothesis and purpose of
EBUS, in addion to a muldisciplinary relaonship between the bronchoscopist and the cytologist.
References:
1. Yasufuku K et al. Chest 2004;126:122–8. hps://doi.org/10.1378/chest.126.1.122.
2. Krasnik M et al. Thorax 2003;58:1083–6. hps://doi.org/10.1136/thorax.58.12.1083.
3. Yasufuku K et al. Lung Cancer 2005;50:347–54. hps://doi.org/10.1016/j.lungcan.2005.07.013.
4. Dincer HE et al. Med Devices Evid Res 2016;9:467–73. hps://doi.org/10.2147/MDER.S62724.
5. Olympus America | Medical | n.d. hps://medical.olympusamerica.com/ (accessed December 20, 2020).
6. Medical Devices for Minimally Invasive Procedures | Cook Medical n.d. hps://www.cookmedical.com/ (accessed December 20, 2020).
7. Boston Scienc- US - Boston Scienc n.d. hps://www.bostonscienc.com/en-US/Home.html (accessed December 20, 2020).
8. SonoTip Pro Control - Medi-Globe GmbH EN n.d. hps://www.medi-globe.de/en/sonop-pro-control.html (accessed December 20, 2020).
9. Medical Technology, Services & Soluons Global Leader | Medtronic n.d. hps://www.medtronic.com/ca-en/index.html (accessed December 20,
2020).
10. Di Felice C et al. J Thorac Dis 2019;11:3643–9. hps://doi.org/10.21037/jtd.2019.04.20
W A B I P N E W S L E T T E R P A G E 6
Boston Scientific
Acquire
TM
Pulmonary
Olympus x x
Medi-Globe
SonoTip® EBUS Pro
Flex
Olympus, Fujifilm,
Pentax
x
Medi-Globe
SonoTip TopGain®
EBUS-TBNB
Olympus, Fujifilm,
Pentax
x
Tips from the Experts
P A G E 7 V O L U M E 9 , I S S U E 1
Introducon
Percutaneous tracheostomy placement for paents with respiratory failure requiring long-term weaning from mechanical venlaon is a
standard pracce in the intensive care unit. The COVID-19 pandemic has brought new concerns regarding the safety, ming, and technique
for tracheostomy placement due to the potenal for transmission to healthcare workers (HCWs). As a result, expert consensus statements
have been formulated and updated as we connue to gain experience with thoughul adaptaons for tracheostomy placement in paents
aected by COVID-19.
Indicaons:
At our instuons, paents who require long-term venlator management and weaning including paents with COVID-19, are considered
for tracheostomy placement. In order to safely perform tracheostomy placement, the paent must be hemodynamically stable and be able
to withstand periods of apnea during the procedure. Ideally, tracheostomy placement will assist hospitals to decompress the intensive care
units and allow for the safe transfer of paents to long term acute care facilies for weaning from mechanical venlaon.
Procedural Consideraons
Planning
When considering tracheostomy placement at our instuons for COVID-19 paents, the following quesons are being addressed.
1.What is the overall prognosis of the paent? Have goals of care been discussed with the paent or family members?
2. How stable is the paent? Is medical opmizaon required prior to tracheostomy for coagulopathy, shock or hypotension requiring high
doses of pressors, or high venlator requirements (>40-60% FiO2 or PEEP 10-14cmH20).
3. Will the team be able to successfully perform the tracheostomy at the bedside? Or should a surgical approach be considered in the oper-
ang room?
4. Is enhanced personal protecve equipment (PPE) available?
5. Which team members are necessary in the room? In our experience with the percutaneous approach, an operator and bronchoscopist
are required along with a respiratory therapist and nurse. Alternavely, an anesthesia team member may replace both the respiratory ther-
apist and nurse during the procedure in order to minimize exposures and conserve PPE.
Technical Guidelines
Recommendaons from consensus statement have been described and summarized below (1,2).
1. Tracheostomy should be considered when prolonged mechanical venlaon is ancipated.
2. Both open surgical and percutaneous approaches for tracheostomy are acceptable.
3. Use of enhanced PPE to migate risk to HCWs is encouraged.
Technique and Timing of Tracheostomy for Paents with COVID-19
Chrisne Argento, MD
Northwestern Memorial Hospital
Ajay Wagh, MD
The University of Chicago

Tips from the Experts
P A G E 8 V O L U M E 9 , I S S U E 1
4. Tracheostomy should be performed in a negave-pressure room.
5. Ulize the least number of providers with the highest level of experience.
6. Maintain closed circuit venlaon while paent is on mechanical venlaon with in-line sucon.
7. Use techniques and equipment with which operators are familiar, condent, and experienced.
8. Encourage the maintenance of a bloodless eld, minimal use of diathermy, and use of smoke evacuator when using an open surgical ap-
proach.
9. Consider a trial of apnea aer preoxygenaon with FiO2 of 100% and PEEP of 5cmH2O to evaluate physiological readiness.
Suggested Timing
The ming of percutaneous tracheostomy placement for paents with COVID-19 has been unclear with insucient evidence for any rm rec-
ommendaons (1). Our instuons follow the suggesons from the published expert panel reports (1, 2).
1. Delay the procedure unl at least day 10 of mechanical venlaon.
2. Consider only when paents are showing signs of clinical improvement.
Due to prior studies demonstrang absence of viral shedding aer 21 days from symptom onset, some groups have suggested waing this
period of me prior to performing tracheostomy. In a single system, mul-center study, Chao and colleagues reported that it is reasonable to
consider tracheostomy before 14 days since they found a (weak) posive correlaon (R
2
0.1382, p=0.04) where paents who underwent ear-
lier tracheostomies tended to achieve earlier venlator liberaon (3). Another study from Avilés-Jurado and colleagues found that the suc-
cessful weaning rate was higher in the early bedside surgical tracheostomy group (<10 days intubaon) compared with the late tracheostomy
group (>10 days intubaon) with no infecons among surgeons idened at the end of the study (4). An analysis of 148 paents who under-
went tracheostomies in the rst 2 months of the pandemic in New York City, showed that early tracheostomy was noninferior to late trache-
ostomy and it did not contribute to increased infecons of clinicians (5).
That being said, there is now data showing that the peak of infecvity of COVID-19 is between day 1- 5 of symptom onset with a signicant
decline aer days 10- 15. Machine learning models suggest that tracheostomy in COVID-19 paents should be considered between days 13
and 17. This is a paent-centered approach as in the rst 12-14 days of mechanical venlaon paents may either be successfully weaned o
the venlator or do not survive their crical illness (6).
Other Suggesons
Best pracces are discussed in detail in the aforemenoned CHEST guidelines (1). Angel and colleagues suggested the use of bronchoscopic
visualizaon alongside the endotracheal tube as a novel method to reduce exposure to aerosol while visualizing proper tracheostomy tube
placement (7). Addional modicaons to the standard percutaneous tracheostomy procedure ulized at our instuons to minimize aero-
sol exposure include:
1. Clamping of the endotracheal tube prior to inseron of the bronchoscope (with the bronchoscope adapter) into the endotracheal tube
as well as minimizing re-entry of the bronchoscope.
2. Draping or covering the face and endotracheal tube and packing the nose and mouth during bronchoscopy.
3. Ulizing manual venlaon with periods of apnea during high aerosol generang moments of the procedure (i.e., when dilang the sto-
ma and during placement of the tracheostomy tube).
4. Occasional assistance from anesthesia colleagues to ensure adequate sedaon and oer hemodynamic support during the procedure to
help minimize addional personnel in the room while maintaining experse with airway, sedaon and mechanical venlaon.
5. We have successfully ulized disposable bronchoscopes for use during tracheostomy (Figure 1), although the subopmal suconing, visi-
bility, and sness of these scopes may be liming factors for an opmal procedure. Studies are needed to conrm the long-term outcomes
of paents who undergo any intervenonal procedure using these disposable devices.
Quality Control
Aer tracheostomy, paents may be transferred to the medical oor once they demonstrate a stable venlator/oxygen requirement or a
long-term acute care facility where ongoing weaning can take place as appropriate. Once the paent is liberated from the venlator, trache-
ostomy decannulaon protocols are followed with modicaons such as maintaining a closed circuit using a heat and moisture exchanger

Tips from the Experts
P A G E 9 V O L U M E 9 , I S S U E 1
(HME) along with a viral lter, minimizing inner cannula or tracheostomy tube changes, and maintaining cu inaon even while o mechani-
cal venlaon unl the paent has either tested negave for COVID-19 or is ready for decannulaon. Any paent noted to have diculty
phonang or breathing following tracheostomy requires a bronchoscopy to evaluate for laryngotracheal stenosis, or obstrucng granulaon
ssue.
Conclusions
The COVID-19 pandemic has complicated roune tracheostomy placement for paents with COVID-19 related respiratory failure due to con-
cerns for increased risk of aerosolized exposure of virus to HCWs. Several adjustments to percutaneous tracheostomy procedural technique
have been proposed to improve safety and have demonstrated success. Professional sociees connue to collaborate to ensure safety for
healthcare workers involved in placement and care of paents requiring tracheostomy.
References:
1. Lamb C et al. Chest. 2020 Oct; 158(4): 1499-1514. PMID: 32512006
2. McGrath B et al. Lancet Respir Med 2020; 8: 717-25. PMID: 32422180
3. Chao T et al. Annals of Surgery. Sept 2020. 272(3): e181-186. PMID: 32541213
4. Avilés-Jurado et al. JAMA Otolaryngol Head Neck Surg. Oct 2020. PMID: 33034625
5. Kwak PE et al. JAMA Otolaryngol Head Neck Surg. Published online December 17, 2020. doi:10.1001/jamaoto.2020.4837
6. Takhar A, et al. Crit Care Explor. 2020; 2 (11) e0279
7. Angel L et al. Ann Thorac Surg. 2020 Sep;110(3):1006-1011. PMID: 32339508
Figure 1: Percutaneous tracheostomy procedure performed at
Northwestern Memorial Hospital ulizing enhanced PPE and
use of a disposable bronchoscope (Ambu ®).
Humanitarian News
W A B I P N E W S L E T T E R P A G E 10
Ethical Issues of Vaccinaon
Sciensts have esmated that 60 to 90 percent of a country's populaon needs to be vaccinated against COVID-19 for coun-
tries to achieve herd immunity and prevent mass future breakouts.
Although tradionally the vast majority of individuals get vaccinaons as recommended, more recently vaccine hesitancy has
increased, mainly fueled by misinformaon through social media but also polical opposions around the world.
Raonal academic analysis clearly show that with any new an-COVID vaccine, serious side eects are extremely rare and
can be detected only aer millions of people are vaccinated. Like in any other vaccine, if those extremely rare events are
detected, society should balance that very low probability of serious reacons with the very real possibility of millions of
deaths related to COVID-19 and/or to the collapse of the health care systems if a large amount of the populaon does not
acquire immunity soon.
But in spite of those obvious benets, many naons could struggle to achieve the required percentage of immunizaon.
In Italy, a study has found that nearly 40 percent of Italians will opt not to take the vaccine. In the UK, a study carried out by
King's College and Ipsos Mori in August 2020 found that just 50 percent of the UK populaon would be willing to be vaccinat-
ed and a similar reluctance has been found in France with 54 percent of people surveyed by Ipos showing that would decline
a vaccinaon. Results of surveys in the US are variable but even the more opmisc do not show more than 60% of the pop-
ulaon would denitely or probably get inoculated.
The potenal harm of these beliefs is that reluctance to get a COVID-19 vaccine could hamper its eecveness.
In 2015, the World Health Organizaon (WHO) declared that the United Kingdom had eradicated rubella and in 2016 it was
designated as measles-free country. Immunizaon rates in UK children were high at that me. By 2016, more than 95% of
the country’s 5-year-olds had received one dose of MMR, and roughly 85% had received the pre-school booster that maxim-
izes immunity. But during the rst half of 2019, Europe had 90,000 cases of measles — more than 17 mes the number re-
ported in the whole of 2016 and several European countries (including the United Kingdom) lost its measles-free status. Sim-
ilarly, the United States, is experiencing a remarkable increase of cases of measles cases since 1992.
Those gures made WHO consider hesitancy to vaccinate as one the ten gravest threats to global health and governments
around the world started to discuss the possibility of adopng policies that would make vaccinaons mandatory. That is be-
cause evidence of vaccinaon’s eecveness is unequivocal and, for instance, Government agency Public Health England
esmates that the measles vaccine combined with mumps and rubella vaccines have prevented 20 million cases of measles
and saved 4,500 lives. In terms of improving public health, vaccinaon is second only to providing clean drinking water.
One of the main factors that explains that relaxed atude towards vaccines is that many people thought that many infec-
ous diseases were relavely harmless. The introducon of some vaccines, has dramacally reduced the number of infec-
ons in the developed world; such reducon, in turn, made invisible to many people the possible severe consequences of
certain infecous diseases and, accordingly, the benets of vaccines. For example, as reported by the Oxford Vaccine Group,
the year before the measles vaccine was introduced in the UK (1967), there had been 460,407 suspected cases of measles in
the country, with 99 measles-related deaths. Aer the introducon of the vaccine, the number of measles cases per year
dropped to around 10,000, with one or two deaths, by the end of the 1980s. Vaccines made and are sll making a dierence.
But in a sense, this success backred: people started to forget, because they could no longer see, that certain infecous dis-
eases can have very severe consequences and even be lethal for certain vulnerable people.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 11
Legal compulsion is a strategy that governments have used previously to overcome such reluctance. In England, the vaccina-
on of all infants was made mandatory in 1853, and parents who failed to vaccinate their children faced nes or prison. Ob-
viously it was a controversial decision as many Brish people consider that it was a raonal way to guard against the danger
of resurgent smallpox, but many others saw a violaon of their bodies and rights. Legal compulsion resulted in a strong an-
vaccinaon movement that resisted the law through protests and demonstraons and that got in 1898 the addion of a
“conscience clause” that excused parents who believed that vaccinaon would harm their children’s health. Unfortunately it
meant that by 1911 only about 56 percent of newborns were being vaccinated. Vaccinaon was also made mandatory in
other European naons as Germany in 1873 aer its experience in the Franco-Prussian War.
In the United States, the rst school vaccinaon requirements were enacted in the 1850s to prevent smallpox. There were
many court challenges from people who considered those policies a violaon of constuonal liberes. Conicng decisions
in these cases culminated in the landmark Supreme Court case Jacobson v. Massachuses in 1905, which held that compul-
sory vaccinaon was a legimate exercise of state governments’ “police powers” to guard the health, welfare, safety, and
morals of cizens. Several federal and state eorts to eradicate measles in the 1960s resulted in many mandates policies. By
the 1990s, all 50 states required students to receive certain immunizaons, and most states required coverage for those in
daycare centers .
Ethical debates and objecons about mandates arise because some individuals and communies disagree with the man-
dates, and/or have religious or philosophical beliefs that conict with vaccinaon. Tension results when individuals want to
exercise their right to protect themselves and/or their children by refusing vaccinaon, if they do not accept exisng medical
or safety evidence, or if their ideological beliefs do not support vaccinaon.
In that context: is there any ethical juscaon for the governments to priorize the common good over individual autono-
my and create policies for mandatory vaccinaon?
There is a large body of literature on the juscaon for the use of coercion in public health, mainly in infecous diseases.
Mandatory vaccinaon is usually jused on Millian principles: harm to others. According to John Stuart Mill, the most
prominent arguments from bioethicists appeal to prevenng harm to others.
In fact, at least two plausible principled juscaons may be oered for mandatory vaccinaon: the harm principle and the
prevenon of free riders.
The harm principle, described by John Stuart Mill in On Liberty, considers that the only juscaon for coercive acon
against an individual is the presence of imminent harm to other members of society. A person’s own good is insucient rea-
son. Those who sustain the legimacy of mandates, point that people who refuse to be vaccinated or to have their children
vaccinated harm others. On the other hand, the counter-argument is that while being vaccinated clearly benets others, it is
less obvious that the failure to be vaccinated harms others as some other factors inuence the likelihood of disease trans-
mission.
The argument that each individual has within his or her power the ability of self-protecon and so can choose to receive a
vaccine, and has no moral claim to force another person to receive it, is extremely weak. Some people cannot undergo vac-
cinaon because of medical contraindicaons or have a diminished biological capacity to develop immunity in response to a
vaccine, not taking into account that no vaccine is 100 percent eecve and some people can receive the vaccine and fail to
develop the intended immunity. All these people may be placed in danger by infecous diseases that unvaccinated members
of the community may spread.
Other potent argument for the use of compulsion is to prevent the problem of free riders, those people who use a public
good without assuming their fair share of the cost. The herd immunity created by high levels of immunizaon can be consid-
ered a public good, by being nonexcludable (if it is available to some people, it must be available to everyone), and nonrival-
rous (the protecon that one individual gets does not diminish the protecon of others). An individual’s self-interested strat-
egy would be to allow everyone else to assume the small risk of vaccinaon but avoid vaccinaon himself and in that way
Humanitarian News
W A B I P N E W S L E T T E R P A G E 12
taking selsh prot of the risks other people have faced.
Regarding to herd immunity Hardin has described the phenomena of the “tragedy of the commons”. In this situaon, the
availability of a shared resource is undermined by self-interested acons. If only one individual refuses vaccinaon, he will
not aect the protecon of the whole community, but if many people make that choice, herd immunity will eventually not
be achieved and the community will stay vulnerable to disease outbreaks.
We many see free riding and the tragedy of the commons as problems of distribuve jusce, in which the benets and bur-
dens of immunizaon are not fairly distributed among all members of society.
Addionally “the clean hand principle” has been described as the situaon in which moral imperave prohibits people from
becoming accomplices in the collecve harm that would result from the failure to achieve herd immunity.
In most of these views, compulsory vaccinaon is jused by the fact that the state has an obligaon to preserve the com-
mon good of herd immunity in order to protect vulnerable people .
In the specic case of COVID-19 the impact of the failure of vaccinaon is not only in terms of deaths from the disease but
also in the enormous economic, health and social consequences of alternave control measures, as lockdown or travel re-
stricons and the unavailability of health care resources for other acute or chronic disease management, consequences
which may be long-term even aer a relave control of the epidemic.
As Julian Savulescu recently described in the Journal of Medical Ethics there is a strong case for making any vaccinaon man-
datory (or compulsory) if four condions are met: a) there is a grave threat to public health, b) the vaccine is safe and eec-
ve, c) mandatory vaccinaon has a superior cost/benet prole compared with other alternaves and d) the level of coer-
cion is proporonate.
As in any ethical analysis, all those variables have to be pondered as it happens with the conict amongst dierent ethical
principal and, consequently, there is always some subjecvity in the given value to each one of them.
Taking that into account, even facing the variaon in tesng rates, and ways of assigning deaths from country to country,
aer months of persistence of the epidemic, there is no doubt that COVID-19 health implicaons may present a grave public
health problem not only as an acute disease but also amongst survivors because of the potenal long-term consequences.
Of course, some will argue that this disease is not “grave” enough to warrant mandatory vaccinaon, compared for instance
with the Spanish inuenza that killed around 50–100 million people and aicted younger rather than older people. The
judgement if COVID-19 is suciently grave requires more data than the available ones, but most of people in the academic
and polical environments would agree that COVID-19 is a grave public health emergency.
The item about the safety of the vaccine is especially sensive as there are concerns that tesng has been rushed and the
vaccine may not be safe or eecve. However, the stascal probability ancipates that no vaccine could be said to be 100%
safe. There will be risks as in any other vaccines and it is not impossible that they will be greater than with well-established
vaccines. But again, the judgement of how much eecve and how much safe it must be to warrant mandatory vaccinaon
will be a maer of discussion. Of course, safety would need to be very high, but a 0% risk opon is realiscally unlikely.
Mandatory vaccinaon must be considered jusable when there are benets to the individual and to the whole community
by prevenng transmission. But an important addional juscaon would be to prevent exhauson of healthcare resources
and to protect other adults who cannot be vaccinated for medical reasons.
Thirdly: has mandatory vaccinaon a superior cost/benet prole compared with other alternaves? In an ideal world, eve-
ryone would want to be vaccinated against Covid and there would be enough vaccine to do that job. We don't live in that
world. Unfortunately the surveys menoned above open doubts about the willingness of the populaon about receiving
COVID-19 vaccine. But addionally, not only reaching herd immunity is important but how fast we reach it in equally im-
Humanitarian News
W A B I P N E W S L E T T E R P A G E 13
portant. A delay in reaching herd immunity may mean tens of thousands of lost lives all over the world. People parcularly
vulnerable (those that cannot be vaccinated for medical reasons or the elderly or chronically sick people) crically depend on
stopping the spread of the disease as soon as possible.
There are other policies that are alternaves to the vaccinaon. They include mainly prolonged or intermient lockdown and
vigorous track and trace programs or enforced quarannes with tracking devices. But on one hand most of those policies
are acvely resisted by the populaon (because of the economic, social and emoonal consequences) and addionally the
long-term costs and benets of such policies are not completely known. It means it cannot be accurately pondered if a man-
datory policy of COVID-19 vaccinaon is ethically jused unl the exact costs of the vaccine, the impact of the problem and
the eecveness of the alternave measures is more sciencally grounded. However, in spite of the lack of denive g-
ures, it is certainly feasible that it could be jused.
If it is considered that coercive vaccinaon can be jused, those who defend freedoms at all costs must admit that, in any
country, there are many other situaons in which mandatory acons exist. In the gravest emergencies, where there is dan-
ger for the whole populaon, people are mandated to take arms to serve their country, in spite of the high risk of death or
permanent injury. Taxes are not oponal to be paid, the use of seat belt or abstenon of alcohol when driving is mandatory.
Even in those countries whose policies favour intervenons of the government as limited as possible, there are public poli-
cies that are mandatory in order to protect and promote the common good.
Mandatory public health policies include any policy that contains a non-voluntary element to vaccine consent. It may be
through the imposion of a penalty or cost for refusal. There are a range of possible penales or costs which can coerce peo-
ple. Australia has the “No Jab, No Pay” scheme which withholds child benets if the child is not vaccinated, and a “No Jab,
No Play” scheme which withholds kindergarten childcare benets. Italy introduced nes for unvaccinated children who
aend school. In the USA, state regulaons mandate that children cannot aend school if they are not vaccinated, and
healthcare workers are required to vaccinate.
Finally, proporonality between the level of coercion and the gravity of the problem should exist. Coercion is jused when
the restricon of liberty is both minimized and proporonate to the expected advantages oered by the more coercive poli-
cy.
The Nueld Council of Bioethics produced an inuenal report on public health which considers when coercion and manda-
tory vaccinaon might be jused: “When assessing whether more direcve policies are acceptable, the following factors
should be taken into account: the risks associated with the vaccinaon and with the disease itself, and the seriousness of the
threat of the disease to the populaon. In the case of incenvized policies, the size of the incenve involved should be ap-
propriate so that it would not unduly compromise the voluntariness of consent.”
The result of this approach is an “Intervenon ladder”, which includes measures as educaon and incenves, as well as co-
ercive measures. In some way it reects the principle of the “duty of easy rescue” : if the cost to an individual is small of
some act, but the benet or harm to another is large, there is a strong moral obligaon to perform that act (the classical
example is “if you noce a child has fallen in and appears to be drowning and to wade in and pull the child out would be easy
but it will mean that you get your clothes wet and muddy, you have the moral obligaon to rescue the
child? As the importance of saving a child so far outweighs the cost of geng one’s clothes muddy and missing a class”).
That principle appropriately balances respect for autonomy with jusce.
Most of experts agree on considering two circumstances in which quasi-mandatory vaccinaon measures are more likely to
be jused. First, for highly contagious and serious diseases and second for disease eradicaon if the disease is serious and if
eradicaon is potenally possible.
Even this summary analysis show that mandatory vaccinaon can be ethically jused but, although it has existed in various
forms for more than 200 years, there is a paucity of good epidemiological studies of the eects of dierent mandates. The
introducon of laws for mandatory vaccinaon is usually accompanied by other measures of educaon and publicity, which
Humanitarian News
W A B I P N E W S L E T T E R P A G E 14
makes it harder to idenfy the specic eects of legislaon. It makes answering the relevant queson whether mandatory
vaccinaon is eecve, a complicated task.
But even taking those confounding variables into account, there is some evidence that mandatory vaccinaon may help. In
the United States, naonwide surveys in the 1970s showed that the incidence of measles was higher in states without man-
dates, and lowest in states where mandates were strictly enforced. Also in Italy and France immunizaon coverage has risen
with the introducon of mandates. And the No Jab, No Pay legislaon withholding state benets in Australia coincided with
full immunizaon rates rising by around 3% allowing to achieve a naonwide coverage nearly 95%.
However the World Health Organizaon considers that persuading people on the merits of a COVID-19 vaccine would be far
more eecve than trying to make the jabs mandatory. Most of data show that the problem is not vaccine refusal, but vac-
cine hesitancy. In most countries, the proporon of the populaon that staunchly opposes vaccines is less than 2% and the
bigger problem is the large group of people with some concerns about vaccinaon that might make them hesitant. It is rea-
sonable to think that the minority of people who refuse vaccines will rarely change their minds but the hesitant populaon,
may respond to informaon campaigns. It would favour a greater investment in educaon and more eorts to facilitate
meaningful conversaons between concerned people and health-care professionals. But every context is dierent and it
must be taken in consideraon that in the last decade the power of mass media and mainly of tools as social media and non-
expert inuencers is increasingly strong and that power is not easily balanced by the tradional communicaon tools of the
governments.
Another problem of the restricve policies is that even being inially very successful, its eecveness vanishes over me. A
study on the eecveness of state-level varicella vaccinaon mandates indicates that “the impact of the mandate is a short-
run phenomenon. The importance of the mandate eect relave to the aggregate me trend (…) is cut by more than a half
by the fourth year aer the mandate and disappears completely approximately six to seven years aer the mandate” .
Coercion may be applied through penales or costs but also through incenves. The dierent types of vaccinaon policies
could be successful in achieving herd immunity, depending on factors such as parcular socio-economic circumstances or
cultural contexts. But deciding which policy to implement should always consider the principles of least infringement and of
least restricve alternave.
The principle of least infringement states that public health authories, when choosing between available policies for achiev-
ing a certain public health goal, should select the health policy that infringes the least upon certain individual rights. Such
rights include the right not to be harmed, the right to receive benecial medical treatments, the right to free movement and
associaon, and the right to bodily integrity and to personal autonomy.
Not only penales may be restricve, the restricveness of any type of intervenon depends on variables of the context of
individuals targeted. Giving nancial incenves might exert a dierent inuence on the decision-making of those who are in
great need of money (for whom is almost impossible to reasonably refuse those incenves) while others might remain in-
dierent to that same incenve.
The principle of least restricve alternave (PLRA) advises to implement the least restricve policy that is eecve, and it
means that governments should test the ecacy of possible policies, starng from the least to the most restricve: persua-
sion, nudging, provision of incenves, withholding of nancial benets, imposion of nancial penales, withholding of so-
cial services and goods and, as a last resort, compulsory vaccinaon. Compulsory vaccinaon should be seen as a measure of
last resort and some of the less restricve opons discussed should be sucient for the realizaon of herd immunity.
Convincing people to vaccinate without coercing them is always preferable, and where some coercion is necessary to
achieve herd immunity, a lower degree of coercion is always preferable. Besides, coercive policies would be necessary only
where outright vaccine refusal is a signicant factor in low vaccinaon rates; where this is not the case, alternave and less
restricve policies such as nudging, improving accessibility and minimizing logisc barriers to vaccinaon are not only ethi-
cally preferable on the basis of the PLRA but probably also very eecve .

Humanitarian News
W A B I P N E W S L E T T E R P A G E 15
As one of the main goals is to limit as much as possible the amount of people who are burdened with restricons on liberty
or autonomy, the governments should grant non-medical exempons to a certain number of people who have deeply held
beliefs against vaccinaon, provided they are not too large a group.
In summary, it can denitely be said that there is a collecve responsibility, or collecve moral obligaon, to achieve herd
immunity and that there is an individual moral obligaon to contribute to the realizaon of herd immunity by being vaccinat-
ed. At the same me, the state has an instuonal responsibility to implement vaccinaon policies that can guarantee at
least the realizaon of herd immunity and the policies should follow the principle of least restricve alternave that would
be eecve in achieving this goal.
On the other hand, a principle of fairness requires that everybody—not just the smallest number of people that can realize
herd immunity—makes their fair contribuon to herd immunity by geng vaccinated. The state is morally jused in requir-
ing each individual to be vaccinated in the absence of legimate medical reasons for exempons; and compulsory vaccina-
on without non-medical exempons is ethically jused.
Even when mandatory vaccinaon can be ethically jused it is quite possible that some mixture of altruism and nancial
and non-nancial benets will obviate the need to introduce mandatory vaccinaon. It is much beer that people voluntarily
choose on the basis of reasons to act well, rather than being forced to do so, and in any case, coercion by incenves is beer
than imposing penales. Educaon, communicaon and structuring the rewards and punishments in a just and fair way is
one way of giving people reasons for acon.
References:
1. Savulescu J. J. Med. Ethics Published Online First: 05 November 2020. doi: 10.1136/medethics-2020-106821
2. Flanigan J. HEC Forum 2014;26(1):5–25. doi:10.1007/s10730-013-9221-5
3. Nueld Council on Bioethics. Public health: ethical issues. London: Nueld Council on Bioethics, 2007: 60.
4. Giubilini A. J Appl Philos 2020;37(3):446–66. doi:10.1111/japp.12400
5. Giubilini A. The ethics of vaccinaon. Palgrave Macmillan, 2019.
6. Nueld Council on Bioethics. Public Health: Ethical Issues. London, 2007
7. Drew L. Nature 575, S58-S60 (2019) doi: hps://doi.org/10.1038/d41586-019-03642-w8. Salmon, D.A et al... Emerging Themes in
Epidemiology. 2006;3:13.
9. Colgrove J. Immunizaon and Ethics: Benecence, Coercion, Public Health, and the State.The Oxford Handbook of Public Health Eth-
ics. DOI: 10.1093/oxfordhb/9780190245191.013.38
*The views expressed in this arcle are those of the author (Silvia Quadrelli) and do not necessarily reect the ocial posi-
ons of the Execuve Board or Internaonal Board of Regents of the WABIP.
Best Image Contest 2021 (1 of 3)
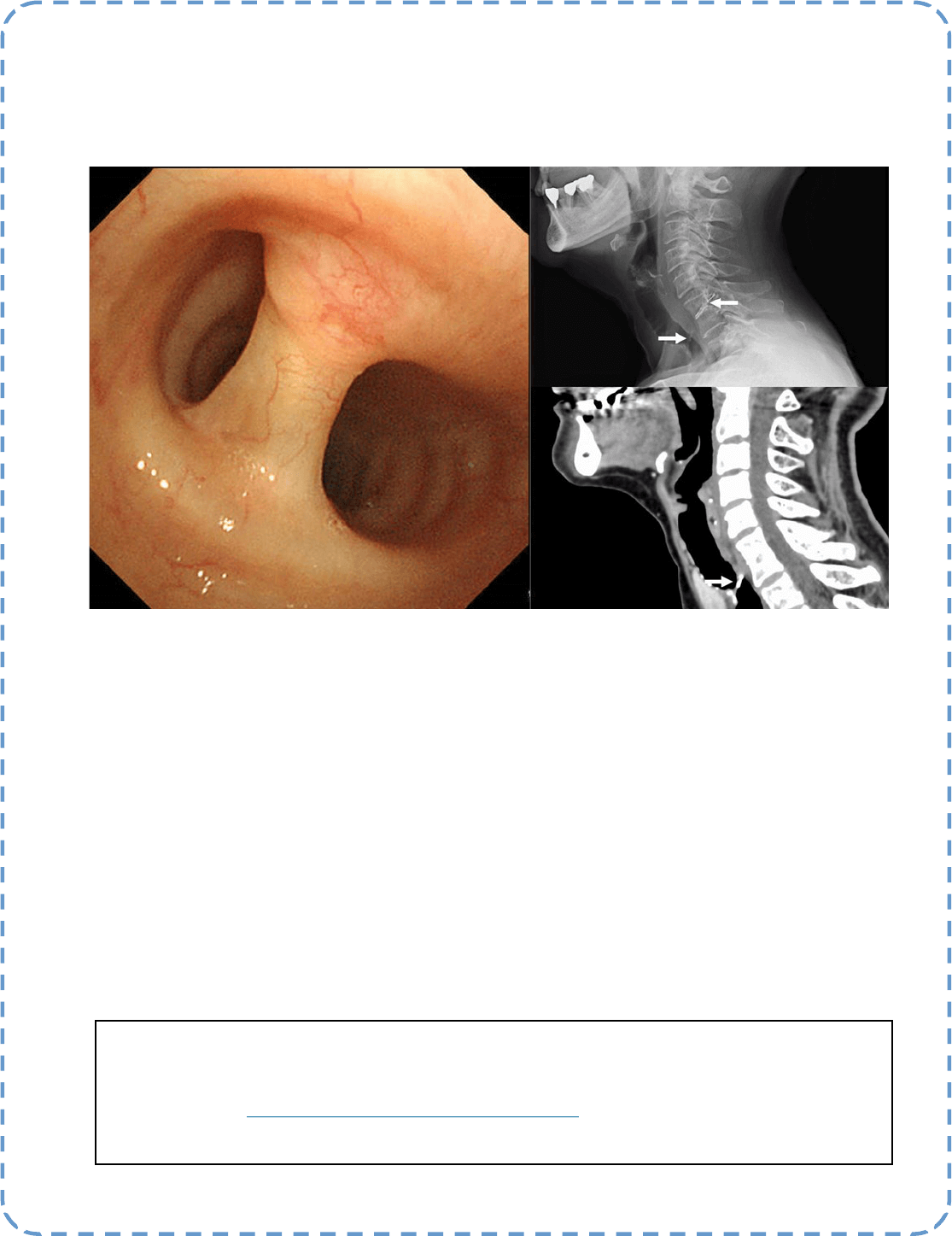
Descripon:
A 74-year-old woman was found to have a foreign body in her trachea during follow-up for a parod tumor. Neck X-ray
and computed tomography revealed a metallic material penetrang the vertebral body and trachea (arrow). Bronchos-
copy showed that the organized material was penetrang the trachea. She had received acupuncture for neck sness
more than 20 years ago, so the foreign body was suspected of being a broken acupuncture needle. The paent had no
complaints related to the foreign body; therefore, we decided to follow the paent.
Best Image Contest
P A G E 16
This image is 1 of 3 selected among 100+ submissions to our Best Image Contest held in late 2020. Please stay
tuned to the next Image Contest opening later this year! Find the above image and more at the WABIP Acade-
my Image Library at hps://www.WABIPacademy.com/imagelibrary
Submier:
Takahiro Nakajima, MD
(Department of General Thoracic Surgery, Chiba University Graduate School of Medicine)

P A G E 17
WABIP News
Annual Board of Regents Meeng 2021
With the new business year, the WABIP Regents (member society representaves) shall meet and vote on
WABIP acvity and nancial reports for our annual lings as a non-prot organizaon in Japan. The meeng
will be held via teleconferencing on MARCH 20, 2021. Regents may also submit their votes to approve our
annual reports and government documents via proxy.
WCBIP 2020 & Beyond
We are very pleased to have successfully concluded WCBIP 2020, amid especially challenging circumstances
before and during the event. This WCBIP proves that running huge virtual events with 35,000+ total parci-
pants is completely possible for the WABIP. We will be using some components of this virtual model as a
basis for our WCBIP events going forward, especially as we strive to include parcipaon from our 10,000
WABIP members from around the world, whether on-site or virtually. See you at WCBIP 2022 in Marseille
France, and WCBIP 2024 in Bali Indonesia!
New Open Commiee Posions
As we begin a new term, a number of new commiee posions are now open. We cordially invite you to ap-
ply for open posions in our: Awards Commiee, Bylaws Revision Commiee, Conict of Interest Oversight
Commiee, or Connued Medical Educaon Commiee. Send your applicaon via hps://
www.wabip.com/forms/commiees
Announcing the 2021 APCB & 2021 ECBIP
Our dear friends and partners at the Asia Pacic Associaon and the European Associaon will be hosng
their biennial events this year, which will both be in October of this year.

Even Perfecon Has Room for Improvement
Appropriate staging of lung cancer is the most crucial aspect of the workup of lung cancer. The proper management and the prognosis hinges upon
the correct stage of lung cancer. Under-staging lung cancer has been a chronic problem leading to sub-opmal therapy, a high “relapse” rate, and
poor outcomes.
We have come a long way in surgical and minimally invasive lung cancer staging with modalies such as Endobronchial Ultrasound (EBUS) guided
Transbronchial Needle Aspiraon (TBNA) of the mediasnal and hilar lymph node. EBUS-TBNA has made lung cancer staging more accessible and
cheaper.
Despite surgical and medical procedural advancements and meculous staging guidelines, the discrepancy between the clinical and pathological
staging of lung cancer persists at an alarming rate.
A recent study (1) evaluated the accuracy of the complete clinical lymph node staging by assessing the agreement between imaging, clinical, and
pathological nodal stage in paents with Non-Small Cell Lung Cancer (NSCLC) eligible for surgery and evaluate the incidence and localizaon of oc-
cult lymph node metastasis (OLM). Three hundred and ninety paents with NSCLC from a single center were studied. The clinical staging based on
CT/PET and lymph node biopsies with EBUS-TBNA or mediasnoscopy were conrmed by nal pathological staging aer anatomical resecon. Any
paent who did not go thru surgical resecon was excluded from the study since their pathological stage could not be veried. Similarly, paents
with enlarged lymph nodes in staon 5 and 6 were excluded since EBUS-TBNA could not evaluate them.
Overall, nal clinical staging corresponded to surgical staging outcomes in 65.5 % of paents.
In the subgroup of paents staged as clinical stage, cN0 (clinically no nodal involvement), 23.1 % had OLM. Paents who underwent staging by
EBUS/EUS were inaccurately staged in as much as 50 % of cases, involving both over staging (39.6 %) and under staging (11.3 %). Remarkably, of all
paents with OLM, 50.0 % had primary tumors ≤30 mm.
The study shows that in the absence of an anatomical parenchymal resecon with systemac mediasnal lymph node dissecon, 23% of paents
with clinical stage N0 would have been undertreated due to the presence of OLM. These paents would have risked being under staged and under-
treated with sub-lobar resecon (segmentectomy or wedge resecon) or non-surgical treatment modalies such as Stereotacc Ablave Radiother-
apy (SABR). Unidened OLM would not only result in missed removal of these involved nodes but could also result in missed opportunies to oer
paents adjuvant chemotherapy resulng in poor outcomes and survival.
Based on this study and many others in the past, OLM is frequently idened in clinically N0 and N1 NSCLC, tumors <3 cm, and oen in regions be-
yond the reach of current staging techniques. These ndings raise a valid concern in paents managed non-surgically (SABR) or with sub-lobar re-
secons since they are never subjected to the nal scruny of pathological staging. It is conceivable that novel therapeuc approaches such as
bronchoscopic ablaon of parenchymal tumors will face similar challenges once they are FDA approved and adapted as mainstream modalies for a
select group of paents.
Our struggles to improve must go on!
Ali I. Musani MD
Editor-in-Chief: Dr. Kazuhiro Yasufuku
Research
Primary Business Address:
Kazuhiro Yasufuku, Editor-in-Chief
WABIP Newsleer
c/o Judy McConnell
200 Elizabeth St, 9N-957
Toronto, ON M5G 2C4 Canada
E-mail: newsleer@wabip.com
P A G E 18
Associate editor:
Dr. Ali Musani
Associate editor:
Dr. Sepmiu Murgu
Reference:
1. Beyaz F et al. Lung Cancer. 2020 Dec;150:186-194. doi: 10.1016/
j.lungcan.2020.10.022. Epub 2020 Nov 7. PMID: 33189983.
P A G E
19
WABIP ACADEMY- WEBCASTS
The WABIP has started a new educaon project recently: THE WABIP ACADEMY. The WABIP Academy will pro-
vide free online webcasts with new and hot topics that will interest pulmonologists and intervenonalists.
Current webcast topic: Tissue acquision for biomarker directed therapy of NSCLC
You can reach these webcasts by using this link: hp://www.wabipacademy.com/webcast/
www.bronchology.com Home of the Journal of Bronchology
www.bronchoscopy.org Internaonal educaonal website for
bronchoscopy training with u-tube and
facebook interfaces, numerous teachiing
videos, and step by step tesng and assess
ment tools
www.aabronchology.org American Associaon for Bronchology and I
ntervenonal Pulmonology (AABIP)
www.eabip.org European Associaon for Bronchology and
Intervenonal Pulmonology
W A B I P N E W S L E T T E R
Links
www.chestnet.org Intervenonal Chest/Diagnosc Procedures (IC/DP)
NetWork
www.thoracic.org American Thoracic Society
www.ctsnet.org The leading online resource of educaonal and
scienc research informaon for cardiothoracic
surgeons.
www.jrs.or.jp The Japanese Respirology Society
sites.google.com/site/asendoscopiarespiratoria/
Asociación Sudamericana de Endoscopía Respiratoria
P A G E 19