Volume 08
Issue 03
September 2020
Inside This Issue
Editorial, 2
Technology Corner, 3-5
Tips from the Experts, 6-8
Humanitarian News, 9-13
Best Image Contest, 14
WABIP News, 15-16
Research, 17-18
Links, 19
Bronchoscopy during the COVID-19 Pandemic
Editorial
WABIP Newsletter
S E P T E M B E R 2 0 2 0 V O L U M E 8 , I S S U E 3
EXECUTIVE BOARD
Silvia Quadrelli MD
Buenos Aires,
Argenna, Chair
Hideo Saka MD
Nagoya, Japan,
Vice-Chair
Zsolt Papai MD
Székesfehérvár,
Hungary, Immediate
Past-Chair
David Fielding MD
Brisbane Australia,
Treasurer
Naofumi Shinagawa,
MD
Secretary General
Hokkaido, Japan
Guangfa Wang MD
Beijing, China,
President WCBIP 2020
Philip Astoul, MD
Marseille, France,
President WCBIP 2022
STAFF
Michael Mendoza
General Manager
Judy McConnell
Administrator
Kazuhiro Yasufuku
Newsleer Editor-in-
chief
P A G E 2
It has been almost a year since the detecon of
the severe acute respiratory syndrome corona-
virus 2 (SARS‐CoV‐2), the virus responsible for the
pandemic coronavirus disease 2019 (COVID‐19).
Beyond the personal and social stresses many of
us are dealing with during this dicult me, we
are also dealing with the strain and changes to
our own healthcare systems. For many of us, this
includes adapng to the changing guidelines re-
garding bronchoscopy and pulmonary interven-
ons. We must take into consideraon the health
of the clinician and healthcare workers in addion
to the paent. We consequently felt it would be
an appropriate me to focus on this in some areas
of this edion of the September newsleer.
The experts from the American Associaon for
Bronchology and Intervenonal Pulmonology
(AABIP) have created and released an ocial
statement on the recommendaons for bronchos-
copy during the COVID-19 Pandemic. As COVID-19
is feasibly transmied during bronchosopy as an
aerosol generang procedure, the statement has
been created to lower the risks to the operator,
support sta and paents in addion to allowing
the ability to carry out the necessary and im-
portant procedures for several diagnosc and
treatment purposes. In summary the suggesons
are as follows:
• PPE: the use of an N-95 respirator (or a pow-
ered air purifying respirator), face shield,
gown and gloves is recommended especially
in both suspected and/or conrmed cases of
COVID-19 or in asymptomac paents in an
area of conrmed community spread
• In areas where community spread is con-
rmed and tesng is available; a nasopharyn-
geal specimen should be obtained prior to
the procedure
• Lower respiratory specimens should be obtained from
endotracheal aspirate or bronchoscopy with bron-
choalveolar lavage to conrm COVID-19 in paents
with severe or progressive disease that require intuba-
on
• The procedure should be completed in a “mely and
safe manner”
• Severity of infecon and the procedure indicaon and
duraon should be taken into account for cases of rou-
ne bronchoscopy in paents recovered from COVID-
19
For further recommendaons it is suggested to read the
arcle in its enrety: hps://www.sciencedirect.com/
science/arcle/pii/S0012369220308503
Following these guidelines can help us to do our jobs in the
midst of this pandemic all while protecng ourselves and
others, achieving our goals and increasing the common
good. If the pandemic has taught us anything, it’s that we
need to think of ourselves as one big unit all trying to ght
this virus together.
Editor-in-chief
Kazuhiro Yasufuku
Technology Corner
Single-use Flexible Bronchoscopes
Introducon
Many endoscopy companies are either developing or have released single-use exible bronchoscopes (SUFBs) with several ad-
vantages over reusable exible bronchoscopes (RFBs) including complete sterility, ease-of-access and portability, providing a cheap
plaorm for o-site bronchoscopic training and research. To date, they have primarily been used in an anaesthec seng where
they have proven to perform to an acceptable and cost eecve level compared to standard RFBs. The few studies on their use in
the pulmonology suite suggest that they are equally ecacious as RFBs in the performance of bronchoalveolar lavage (BAL) whilst
their use will undoubtedly extend to more complex intervenonal procedures with ongoing improvements in handling, channel
size, angles of deecon and image quality.
Background
The outbreak of nosocomial infecon secondary to contaminated RFBs is a well-documented phenomenon. The most prevalent
infecous agents in these scenarios are mycobacteria and Pseudomonas aeruginosa (1). Though previously, the majority of these
infecons were linked to breaches in the reprocessing guidelines, recent evidence showed residual proteins and potenally infec-
ous pathogens on RFBs that were ready for paent use despite complete adherence with reprocessing procedures (2). The dis-
ease-causing potenal of the organisms in this scenario has not been denitely established but obviously, the risk of transmission
is of concern. SUFBs are sterile and thus eliminate this risk enrely. The COVID-19 pandemic has refocused bronchoscopy units on
the nosocomial and health care provider infecon and the reduced handling required with SUFBs means that health care organisa-
ons are recommending their use in cases of suspected or conrmed COVID-19 (3, 4).
One would expect that SUFBs are a more expensive alternave to RUFBs, however when the cost of cleaning materials, mainte-
nance of automated endoscope reprocessors (AERs), personal protecve equipment (PPE) and wages for reprocessing sta is in-
corporated with the cost of treang potenal infecons arising from residual organic material on fully reprocessed RFBs they have
in fact, been shown to be more economical (5).
Clinical Applicaons
SUFBs have been studied in an anaesthec seng with regard to the placement of endotracheal tubes, use in unancipated di-
cult intubaons and for bronchial sampling and have been shown to be acceptable compared to RFBs in these sengs (3). One
study concluded that SUFBs were comparable to RFBs in cell yield and viability in BAL samples from healthy volunteers (6). Data is
lacking at present regarding their performance for more advanced procedures such as biopsy and transbronchial needle aspiraon
(Figure 1).
W A B I P N E W S L E T T E R
P A G E 3
Dr. Sarah Barron MB BCh BAO MRCPI,
Respiratory Registrar, Cork University
Hospital
Dr. Marcus Kennedy MD FRCPI
FCCP,
Consultant Respiratory Physician,
Intervenonal Pulmonologist,
Cork University Hospital

However SUFBs have a number of characteriscs that prove advantageous for certain clinical and non-clinical applicaons and scenarios
(Table 1).
Ease of Mobility
The scope and portable monitor are light and portable and thus reduce sta and me requirement for moving equipment out of bronchos-
copy units to other healthcare sengs.
Praccality
Having SUFBs readily available reduces the requirement for sta to clean and prepare bronchoscopes which is especially important in out-
of-hours, night and weekend bronchoscopy where RFBs may not be readily available. The impact of cleaning sta absence due to for in-
stance COVID-19 outbreak would therefore not impact bronchoscopy list. Full airway inspecons are oen required but not feasible with
current EBUS convex probe bronchoscopes and having access to SUFBs in this scenario precludes the requirement for RFBs to be ready in
case they are needed.
Specic Scenarios where Reduced Risk of Cross Infecon is Crical
Many hospital protocols require decommissioning of bronchoscopes used in paents with suspected prion disease. Severely immunocom-
promised paents represent another group where SUFBs may have advantage.
Other Applicaons
The cost of shipping bronchoscopes and processors to temporary locaons is signicant. O site, cadaveric, bench and large animal re-
search are ideal scenarios for SUFBs where researchers and trainers require scopes on a temporary basis.
Whether or not a SUFB will be as ecient as an RFB in more complex procedures such as transbronchial needle aspiraon (TBNA) or cryobi-
opsy has yet to be determined. Many of the companies developing SUFBs are now on third and even fourth generaon devices with im-
provements in handling and angle p deecon with each generaon. Areas of concern regarding more complex procedures might arise
from the uniformity of the inner diameter in SUFBs and whether this might compromise more complex procedures. Addionally, previous
studies in an anaesthec seng have suggested that previous SUFBs image quality were not equivalent to RFBs (3) however scope develop-
ment will in no doubt lead to improvements. Larger trials invesgang the reliability of SUFBs in performance of standard biopsy proce-
dures are required.
Conclusion
SUFBs have been on the market now for approximately ten years with research and development improvements being considered with
each new generaon of device. They have proven to be acceptable for mulple anaesthesiologist-led procedures and in a research seng
for BAL. They have several advantages owing to their sterility, easy portability and the potenal for immediate access to the technology. As
well as this, there is mounng evidence that they are a more economical alternave to RFBs – a pernent issue when cost analyses can
limit access to healthcare resources. However, as with any single-use technology, whether or not they will funcon to a sasfactory level in
more complex procedures where imaging quality and uniformity of materials may have a small but incremental impact on outcomes has
yet to be determined.
W A B I P N E W S L E T T E R P A G E 4
References:
1. Kovaleva J et al.. Clin Microbiol Rev. 2013; 26(2): p. 231-54
2. Ofstead CL et al. Chest. 2018; 154(5): p. 1024-1034
3. Barron S et al. J Bronchology Interv Pulmonol . 2020 Apr 17;10.1097/LBR.0000000000000685
4. Wahidi MM et al. J Bronchology Interv Pulmonol. 2020 Mar 18. doi: 10.1097/LBR.0000000000000681
5. Mouritsen JM et al. Anaesthesia. 2020; 75(4): p. 529-540
6. Zaidi SR, et al. BMC Pulm Med. 2017 May 05; 17(83)
Table 1: Clinical and other scenarios where Single Use Flexible Bronchoscopes (SUFBs) have advantages over Reusable Flexible Broncho-
scopes (RFBs).
Ease of Mobility Praccality Specic Scenarios where
Reduced Risk of Cross Infecon is
crical
Other Applicaons
ICU Bronchoscopy Out of hours bronchoscopy Immunocompromised paent Bronchoscopy Training
Emergency Department/ Ward
Bronchoscopy
End of day list-sta are not
required to stay and clean
scopes
Prion Disease Veterinary Procedures
Emergency Bronchoscopy
outside Healthcare Facility
Weekend bronchoscopy where
sta are not available to clean
scopes
Large animal or
cadaveric research
Bronchoscope available for
airway inspecon with EBUS
procedures
W A B I P N E W S L E T T E R P A G E 5
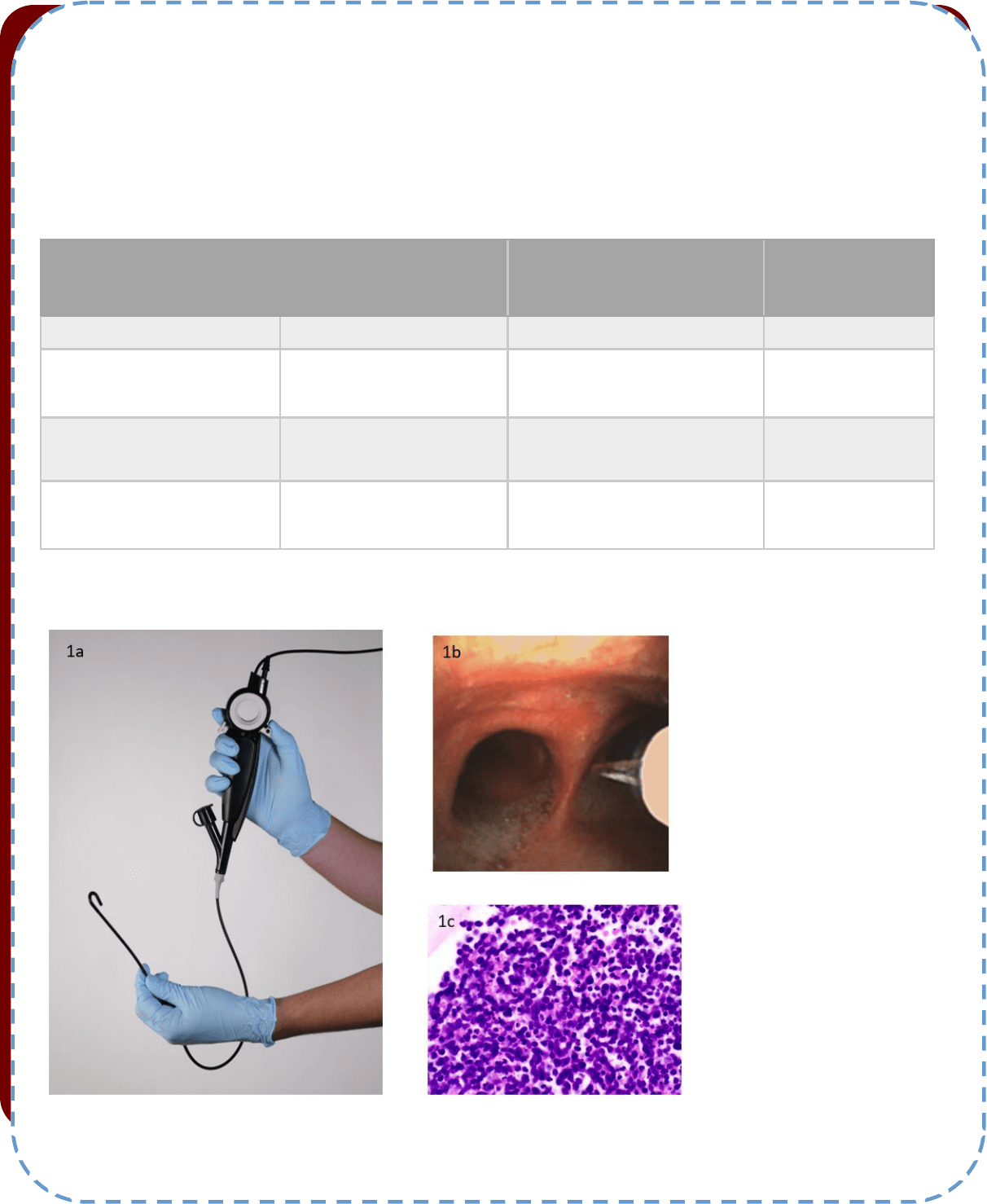
Figure 1: Transbronchial needle aspiraon
(TBNA) using a single use exible broncho-
scope (SUFB) in a 66 year old male with
mediasnal adenopathy
1a. A single-use exible bronchoscope (The
Broncoex® Agile from Axess Vision
(Reproduced with permission))
1b. Endobronchial image of TBNA from
staon 7 subcarinal node using The Bron-
coex® Agile SUFB.
1c. TBNA sample displaying small cell lung
cancer (H and E 400x).

Tips from the Experts
P A G E 6 V O L U M E 8 , I S S U E 3
Introducon
Bronchoscopy plays a crical diagnosc and therapeuc role in a variety of lung disorders but is considered an aerosolizing procedure and
potenally poses a high risk of viral exposure to healthcare workers and other paents in the periprocedural areas. As the COVID-19 pan-
demic connues to cause signicant morbidity and mortality throughout the globe, healthcare providers struggle to balance the philosophy
of mely care with that of safety. Eorts are focused on liming the risk of exposure of SARS-CoV-2 to paents and healthcare workers.
While data specic to bronchoscopy during the COVID-19 pandemic is scarce, various professional pulmonary sociees have provided guide-
lines on how to safely perform bronchoscopy amidst a pandemic.
Paent Selecon
Professional sociees have emphasized the importance of reviewing the need for all bronchoscopic procedures on a case-by-case basis and
have outlined recommendaons for ming the bronchoscopy based on its acuity (emergent, urgent or non-urgent). Some categorized bron-
choscopies in ve groups: emergent (same day), urgent (1-2 days), acute (within 2 weeks), subacute (aer 2 weeks) and elecve (reschedule
when possible). We believe that there is no substute for good clinical judgment and that the priorizaon of a procedure has to consider
the associated comorbidies, procedure factors (duraon, probability of hospitalizaon/ ICU stay) as well as the disease factors which in-
clude the availability and eecveness of non-bronchoscopic opons and the impact of a 2-week or 6-week delay on disease outcome. In
these regards, surgeons at the University of Chicago have validated a scoring system accounng for all these variables when priorizing
medically necessary, me sensive procedures.
Emergent bronchoscopies are easy to dene as they warrant intervenons within hours. These include but are not limited to processes that
cause acute or impending respiratory failure: acute foreign body aspiraon, massive hemoptysis without a clear source for embolizaon,
airway stent migraon, tracheoesophageal stula with evidence of ongoing aspiraon, persistent air-leak in a paent who is unable to ven-
late, and crical central airway obstrucon. The challenge is to disnguish between the bronchoscopies that have to be performed within a
couple of weeks and those that can be deferred for 4-6 weeks. Diagnosis and staging of lung cancer via bronchoscopy fall within these cate-
gories, urgent or non-urgent depending on tumor size, locaon, nodal involvement and tumor biology. In these regards, published evidence
suggest that the risk of upstaging NSCLC signicantly increases aer delays of approximately 6 weeks. In addion, medical oncologists con-
sider the use of neoadjuvant or rst line chemotherapy in newly diagnosed lung cancer as a high priority. In the ESTRO/ASTRO statement,
there was a strong consensus (96%) among radiaon oncologists not to delay iniaon of treatment (by 4-6 weeks) for locally advanced
stage IIIA (bulky N2) NSCLC or to delay palliave radiotherapy for NSCLC.
In view of these recommendaons, we believe that as far as lung cancer is concerned, diagnosc and staging bronchoscopy should NOT be
deferred in the following scenarios:
• Solid or predominantly solid lung nodule suspected of lung cancer >2 cm
• Suspicion for N2/N3 node-posive lung cancer
• Conrm stage II for neoadjuvant chemotherapy
• Conrm stage III for neoadjuvant chemotherapy
• Conrm stage III for denive chemoradiotherapy for inoperable paents
• Conrm limited stage small cell lung cancer for chemoradiotherapy
Praccal ps for performing bronchoscopy for diagnosis and staging lung cancer
during the pandemic
Sepmiu Murgu MD, FCCP, DAABIP
University of Chicago
Elliot Ho, DO
University of Chicago
Tips from the Experts
P A G E 7 V O L U M E 8 , I S S U E 3
• Obtain ssue for diagnosis, NGS/PD-L1 to iniate 1st line therapy for advanced disease
• Conrm symptomac progression of disease for second line treatment
Paent evaluaon prior to bronchoscopy
Guidelines from various sociees recommend broad screening for COVID-19 in order to reduce the risk of infecon transmission. Paents
should be asked about symptoms, contacts, and travel history prior to scheduling and again prior to arrival for planned bronchoscopy. If the
paent has increased risk factors or signs and symptoms of acve viral infecon, the procedure should be delayed if possible.
SARS-CoV-2 RNA tesng within 72 hours prior to the procedure is now rounely performed in many instuons. Paents are also instructed
to self-isolate between the me of tesng and me of procedure. In paents with negave results, bronchoscopy can proceed with enhanced
personal protecve equipment including either N95 mask or PAPR, face shield/googles.
Virus prevenon measures before and aer the procedure include social distancing, video-visits, screening exposed providers, universal
masking in the hospital and limitaon of visitors.
In paents with posive COVID-19 results, it is recommended to postpone all non-emergent bronchoscopies. The me of rescheduling the
bronchoscopy depends on the outcomes of the disease as well as esmated duraon of viral shedding. In paents with conrmed COVID-19
infecon who recover and need a roune bronchoscopy, the AABIP/CHEST expert panel report suggest the ming of the procedure is cus-
tomized based on the indicaon for the procedure, the severity of the COVID-19 infecon and me from symptom resoluon. It would be
reasonable to wait at least 30 days from resoluon of symptoms with negave SARS-CoV-2 RNA tests from at least two consecuve nasopha-
ryngeal swab specimens collected ≥24 hours apart, but this may not be feasible in paents with suspected lung cancer at high risk for upstag-
ing, disease progression or who need immediate iniaon of radiaon or systemic therapy.
Personal protecve equipment
Frequent hand washing is the single most important intervenon and should be performed before and aer touching any equipment needed
for intubaon or bronchoscopy. Personal protecve equipment including gowns, masks, eye shields, and gloves should be worn during all
bronchoscopic procedures (Figure, boom panel). Healthcare workers are recommended to maximize their level of protecon by using either
N95 mask or PAPR when performing an aerosol-generang procedure. The CDC recommends aerosol-generang procedures such as bron-
choscopy be performed in negave pressure rooms when feasible. Liming the personnel in the room to essenal healthcare workers may
also reduce the risk of viral exposure and transmission.
Bronchoscopy in suspected or conrmed COVID-19 infecons
Bronchoscopy should be postponed in paents with highly suspected or conrmed COVID-19 infecon unless there is an emergent or urgent
indicaon. Although the sensivity of BAL is reportedly 93% as compared with the sensivity of nasopharyngeal swab of 63% in detecng
COVID-19 as per a recent study from China, bronchoscopy should not be used rounely to diagnose COVID-19. Upper respiratory specimens
such as nasopharyngeal swab should be the rst-line tesng modality for COVID-19 tesng. Lower respiratory tract specimens via ET aspirate
or bronchoscopy may be considered in paents with severe progressive respiratory failure aer two negave upper respiratory specimens
and addional specimen is needed to establish a diagnosis that will lead to a change in clinical management.
In paents with suspected or conrmed COVID-19 who require emergent or urgent bronchoscopy, it is recommended that healthcare work-
ers in the procedure and recovery room use full personal protecve equipment and N95 mask or PAPR. Extended use and reuse of N95 mask
is not recommended when performing a bronchoscopy in these paents.
Certain technical ps during the bronchoscopy could potenally reduce the risk of aerosolizaon. These include: performing bronchoscopy
via an endotracheal tube, having paents under general anesthesia with neuromuscular blockers to allow for intermient apnea during the
actual suconing, preoxygenaon with 100% FiO2 and ulizaon of disposable scopes for simple therapeuc aspiraons, BAL or for percuta-
neous tracheostomy. Disposable bronchoscopes are likely inadequate for complex bronchoscopic procedures and we believe are subopmal
for diagnosis of peripheral lung lesions and not an opon for mediasnal staging.
Procedural consideraons
In paents who require bronchoscopy, every eort should be made to minimize the me of aerosolizaon to reduce the risk of transmission.
It is recommended that the most experienced operator perform the procedure and personnel be limited to a minimum (Figure, boom pan-
el). Pernent to lung cancer diagnosis and staging, at the University of Chicago, we have connued to use the cytopathology team for rapid
on-site cytology evaluaon to potenally decrease the me of the procedure and to assure sucient material for molecular studies.
Tips from the Experts
P A G E 8 V O L U M E 8 , I S S U E 3
Intubang a paent prior to bronchoscopy oers the advantage over moderate sedaon in that it allows for a closed circuit and potenally
decreases coughing which has been associated with increased aerosolizaon. While intubang a paent prior to bronchoscopy, every eort
should be made to limit bagging during the pre-oxygenaon phase and aer the endotracheal tube is placed. Our team has used intubaon
boxes in the beginning of the pandemic, but now our anesthesia colleagues rounely use only video-laryngoscopy (Figure, top panel). Once
intubated, a HEPA lter should be placed between the endotracheal tube and the venlator circuit to lter out viral parcles. Pharmacologic
intervenons such as paralycs may be considered to decrease coughing.
It is suggested that the number of mes removing and reintroducing the bronchoscope into the endotracheal tube be kept to a minimum in
order to minimize interrupon of an otherwise closed circuit. Although there is no data to support this pracce, acve suconing can be used
during inseron and removal of the bronchoscope from the endotracheal tube in order to decrease aerosolizaon.
Conclusion
We have highlighted some lessons learned during the last 6 months and summarized recommendaons from various sociees on the topics
of paent selecon, paent screening, and procedural consideraons, with the focus on bronchoscopy for diagnosis and staging of lung can-
cer. In the midst of the pandemic, it has become more important than ever for the bronchoscopist to carefully weigh the need to deliver
mely care to paents while lowering the risk of infecon transmission to healthcare professionals and other paents. We trust that the data
from bronchoscopy studies during COVID-19 will allow physicians to again align the philosophy of safety with that of mely and eecve
care.
References:
1. Prachand VN et al. J Am Coll Surg. 2020 Aug;231(2):281-288.
2. Guckenberger M et al. Radiother Oncol. 2020 May;146:223-229.
3. Wahidi MM et al. Published online ahead of print, 2020 May 1]. Chest. 2020;S0012-3692(20)30850-3. doi:10.1016/j.chest.2020.04.036
4. Pritche MA et al. J Thorac Dis. 2020;12(5):1781-1798. doi:10.21037/jtd.2020.04.32
5. Lentz RJ et al. Respirology. 2020;25(6):574-577. doi:10.1111/resp.13824
6. Wang W et al. Published online ahead of print, 2020 Mar 11]. JAMA. 2020;323(18):1843-1844. doi:10.1001/jama.2020.3786
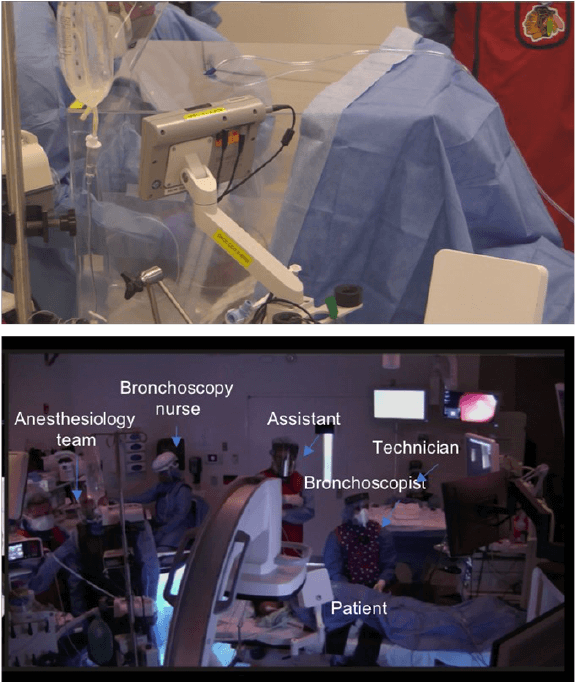
Figure 1: Room set up during a roboc bronchoscopy
during COVID-19.
Top panel: the intubaon box and the video-
laryngoscope used to minimize aerosolizaon during the
intubaon.
Boom panel: room set up and team wearing gowns,
masks, eye shields, gloves and either N95 mask or PAPR.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 9
DUTY OF CARE: PROFESSIONAL OBLIGATION OF HUMAN MORAL CHOICE?
Throughout history, several lethal pandemics have challenged humankind. Two major causes of death are recognized: the
lethality of the disease itself but also the disrupon of basic health care, public health and public safety infrastructures. Dur-
ing the several epidemics lived in the last decades, many ethical issues have been analyzed: the right of governments to re-
strict some liberes in dierent forms of lockdown, the allocaon of limited resources, the equilibrium between individual
rights and the protecon of the whole community, the responsibility of the governments in providing adequate resources.
However, in many publicaons from the press or from scholars in ethics or medicine, it seems that the “duty of care” of
health care workers (HCW) is out of discussion. It has been argued tradionally that the special commitment of doctors to a
high standard of altruism and benecence (and consequently) to a duty to care even at risk to themselves, is one side of the
social contract between the profession and society at large. And that taking risks is just “part of the job”.
However, far from being a subject with high levels of agreement, the denion, the extent, the origins and the very exist-
ence of a duty of care is a maer of great controversy amongst praccing doctors and scholars of ethics.
The disposion to work in the case of a potenally lethal infecous disease has been invesgated in several studies during
previous outbreaks. In a Taiwanese survey performed during the severe acute respiratory syndrome (SARS) epidemic in
2003, 26% of nurses declared they would look for another job or considering resigning because of risk. Other survey, also in
Taiwan, showed that 57% of nurses indicated that they were willing to care for paents infected with avian inuenza. One
study amongst US physicians, showed that only 40% announced that they were willing to put themselves at risk in order to
save others’ lives and other in Maryland, demonstrated that nearly half of the local health department workers would not to
report to duty during an inuenza pandemic. A German study showed that 28% of the respondents HCWs of large terary
centres agreed that it would be professionally acceptable to abandon their workplace during a pandemic to protect them-
selves and their families and 19% of healthcare workers at the Nongham University Hospital NHS Trust in the United King-
dom said they would leave work in the case of a high-lethality infecous disease.
In fact, a working group gathered to idenfy the key ethical issues of the SARS epidemic in Toronto could not reach consen-
sus on the issue of duty to care, parcularly regarding the extent to which healthcare workers are obligated to risk their lives
in delivering clinical care.
Used in a vague, ill-dened, authoritave manner, the phrase duty of care might be ethically dangerous. As pointed by Sokol,
it could pressure HCWs into working in unacceptably risky condions while presenng the ”illusion of legimate moral jus-
caon” . It has been proposed that the duty to treat denion should be narrow and unambiguous in order to allow to
establish with certainty when it does and does not apply. That assignment is not an easy task. Such a denion should take
into account the expectaons of the dierent physicians according to their choice about place and type of work, the abstrac-
ons of the ethical codes, the expectaons of the society (frequently based on many unrealisc assumpons) and, very im-
portantly, the consideraon of how to handle the duty when it conicts with one or more other dues with greater moral
force.
Almost every physician assumes a primary ethical duty to place the welfare of their paents above their own interests. But
how far does the duty to paent welfare extend? Must physicians assume a serious risk to their own health to ensure that
paents receive needed care?
Every country may have parcular rules as those dictated by the common law and codes of ethics (somemes referred to as
an instrument of "so law," owing to its non-legislave nature). But those regulaons are not universal. On the other hand,
the moral grounds of a duty to care concern to HCWs all over the world.
One of the assumpons of members of the society and many physicians is that this duty of care “has always existed”. But
this concept is wrong. No explicit menon is made about such an obligaon in Thucydides or Hippocrates and it is well
Humanitarian News
W A B I P N E W S L E T T E R P A G E 10
known that Galen ed from Rome during the Antonine plague in the second century A.D., Sydenham from London in the
seventeenth, and recognized physicians in Philadelphia and New York during outbreaks of yellow fever in the eighteenth and
cholera in the nineteenth centuries.
Many physicians at those mes, although not expected to pracce in plague areas, chose to stay. But professional duty was
not the reason why they did so. During the plagues of the Middle Ages, the civic leaders of the cies used a variety of poli-
cies, oen in concert or in sequence, to insure minimum levels of palliave treatment for most of the populaon. Physicians
were somemes forbidden to leave some cies and their hinterlands. But fundamentally, they were oered high fees and
prizes to visit paents in the lazere (plague hospitals) and to serve in the hospital. The city leaders and physicians saw
these combinaons of incenves and disincenves to treat paents with plague simply as business proposions. As such,
they were regulated by contracts not very dierent from the commercial instruments used to regulate other commercial
acvies and that expressed the mutual self-interest of a physician and a city: high salaries, reimbursement for living expens-
es and the promise of cizenship in exchange to visit plague paents as frequently as necessary. In more modern history we
nd analogies to events in London during the outbreaks of plague in the seventeenth century and Americans reacted similar-
ly in similar situaons. It means than the history of “duty” to care meant many physicians' incomes improved during epidem-
ics. Plague doctors performed the most dangerous tasks, but they were amply rewarded in cash and if they survived, in the
more important coin of social and professional status.
On the other hand, during medieval mes the duty was no doubt linked with religious obligaons, such as the duty of Chris-
an charity, whereas the 19th century physician adhering to the Thomas Percival’s Code of Ethics might have been movat-
ed by more secular noons of the “gentleman physician”.
It was not really unl the 1800s when the noon of professions as holding a social contract came. The AMA Code of Medical
Ethics version of 1847, specied this professional duty to treat in the face of personal danger which was strengthened in
1912 “to say there was an obligaon to connue taking care of people who posed a contagious threat, even if you were not
being paid to do so,” Even when that Code (very inuenal but not valid in most of the other countries) contributed to build
the image of doctors as a sort of heroic gures in American culture, it is well known that this document evolved to dierent
formats that stressed dierently about that parcular topic along the years.
This means that the duty to treat cannot be rmly grounded on facts of medical history. So, accepng that “tradion” is not
the incontestable argument of a “natural”, intrinsic duty which many authors rely on, but the result of negoaons, religious
movaons and fundamentally, dierent historical contexts, it is mandatory to menon the ethical grounds used as argu-
ments for those convinced of the existence of a duty to care.
The main reasons argued for the existence of a duty to care are (1) an explicit or implicit consent to accept such risks as part
of a professional career in medicine; (2) part of the oath or code of ethics that HCWs undertake when they enter the profes-
sion; (3) special training and experse that give physicians a higher responsibility and (4) a social contract with the public in
return for receiving benets such as subsidized training, high income, social presge and the privilege of professional self -
regulaon and autonomy.
Although each one of those points may be (and have been) quesoned by dierent ethicists, It is far beyond a short column
like this to explore in depth every line of reasoning. Let’s menon however than not in all (and probably not in any) profes-
sional oath is explicitly told that a physician must face potenally lethal risks. The current generaon of physicians has expe-
rienced very lile exposure to serious occupaonal risk. Control of infecons have made doctors in developed countries be-
lieve (with some juscaon) that they are exempt from the riskier aspects of medicine that had claimed the lives of so
many of their predecessors. As the result of that pax anbioca, being a doctor did not mean at all that one was willing to
take personal risks for the benet of paents. Any doctor entered the profession with a keen appreciaon of the hazards.
Only during the last decade, reality abruptly changed, vanishing this percepon of relave safety. Most of contemporary
doctors have pledged to full this singular responsibility of defending the interests of their paents ahead of their own per-
sonal interests but not expecng to include facing life threatening risks.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 11
Some ethics scholars have gone very far in those arguments and so Masur et al wrote that “… physicians and nurses have an
obligaon to treat sick and potenally infecous paents because they are members of a profession whose primary goal is
an ethical calling: caring for the sick. This obligaon to serve the sick is constuve of medicine as a profession and is unique-
ly what disnguishes physicians, nurses, and other clinicians from other professionals” meaning that avoiding risky paents
is a basic betrayal of professional identy. An argument very dicult to be sustained in front of the fact that many doctors
probably having chosen speciales because they do not carry special risks have very dierent expectaon than those who
have taken those that carry well known risks with them. The argument have also several weaknesses, as in any society many
dierent groups have special skills with special essenal goals and are not required to take that level of risk and if they are,
they easily reject to comply with those supposed expectaons on behalf of their freedom of choice and their right to pre-
serve their own lives (or even properes).
A classic argument is that “a physician is like a reghter, they cannot excuse themselves from from entering a burning
building to search for those trapped inside”. You can’t be a reghter if you can’t serve the mission; and that mission carries
to be prepared to take substanal risks.
The analogy proves to be weak. At entering the profession, reghters (or policemen or soldiers) know the sort of risk they
will face. But addionally, their duty implies to be ready to take certain level of risk, not any level of risk. Even for profes-
sions that carry an intrinsic high risk of death, the duty is not applied to risks much higher than the average, known and ac-
cepted by a member of the profession. A police ocer is not obliged to stop armed thieves in a car robbery that is not imply-
ing potenally lethal harm for human lives if he himself is unarmed and for a soldier joining a squad bomb is a volunteer
task, not compulsory to be accepted by every member of the Army.
Finally, one cannot deny that the “social contract” between society and doctors is quite eroded, especially in some countries.
It has been argued tradionally that the special commitment of doctors to a high standard of altruism and benecence, and
hence to a duty to care even at risk to themselves, is one side of the social contract between the profession and society at
large. Contracts oer benets in exchange for services rendered: the benets doctors seek in exchange for recognizing a
duty to care have been proposed to be self-regulaon, or the high status and generous remuneraon of the profession.
Some authors remark that the seless service of doctors during epidemics is perhaps not as seless as it appears: and under-
stand this ‘seless service’ as something of a bargaining tool, in which doctors bargain for their status as independent prac-
oners, self-regulang, and beholden to no outside social body.
But, the concepon of a physician as a “privileged cizen” is no more than a caricature of the past. In most of the countries,
physicians (and not menoning nurses and other HCWs) receive much lower salaries or fees than in the recent past and then
those received by non-essenal professions. The supposed independence of doctors in the regulaon of their pracce does
not exist anymore. The generalizaon of third-party payers have transformed the majority of praccing doctors in informal
employees with no social benets who do not decide their fees, their hours of pracce their working condions and even
their choice of methods of diagnosis and treatments. But most of all, the presge of the medical profession itself has been
corroded (by many factors) and today, doctors are frequently vicms of manifestaons of disrespect, discriminaon and
verbal or even physical violence. Doctors feel today that they have endless obligaons and virtually no rights, just because of
being a physician.
However in spite of the many reasons HCWs have to dispute and even reject that supposed duty of care, most of physicians
have willingly accepted to take risk for them and their relaves and stay at the front line. There is lile doubt that the vast
majority of HCWs performed their jobs admirably. Why? Obviously, the factors playing into ethical decision making are not
exhausted by an ‘implicit contract’ dened by past risk level accepted. A debate about duty to care in the context of an epi-
demic asks whether it is fair to expect of healthcare workers that they take on a risk of personal injury or death and the bur-
den of psychological stress associated with that risk in order to provide care.
If we can’t say that caring for these paents is a basic duty shared by all professionals, it doesn’t mean we can say nothing.
When we set the language of duty to one side, we can say something dierent: that the willingness to care for risky paents
is a very good and seless thing, which exemplies the highest ideals of the profession.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 12
Probably the duty to treat is grounded mainly in an empathic response to the paent’s medical need and vulnerability. Lack-
ing medical knowledge, the sick stand in a relaon of dependency toward those with the power to heal them. As the unique
possessors of medical skills, physicians hold an awesome and exclusive power, through their acons and omissions, to pro-
foundly aect the lives of others. This combinaon of extreme vulnerability and exclusive power in the context of the physi-
cian-paent encounter generates a strong duty, a moral responsibility. We may also think that the duty is also grounded on a
shared ideal of medicine as a profession dedicated to the good of others, a profession which has always had within it mem-
bers who have persistently seen themselves as more than merely self-interested tradesmen.
This noon implies a huge dierence, the dierence between being obliged to do something and making the choice of doing
something. A virtuous act is the elecon of a virtuous man. Not stealing a poor person is an obligaon, giving money to
someone in need is a personal choice. Physicians can be drawn to ideals even when they’re not driven by dues.
But accepng the free intervenon of the physicians as a moral agent also shows its own complexies. Some quesons like
who denes which virtues are required in a physician, which are the limits of that moral duty or how to solve the conicng
dues of a physician’s (to himself, to his family and to the whole society) are not so easy to answer.
Virtues are not universal meless values, but shaped by a historical context. The shape of the professional obligaons has
been determined over me through negoaon with society. The negoaon is complex because it should be based on the
requirement of a common morality. The physician’s duty to take risks has been forged in an ongoing dialogue with society at
large. Taking that into account, it should be accepted that the fact that virtuous physicians behaved one parcular way un-
der condions exisng long ago must not necessarily reect the concept of virtue today. Many things about medical pracce
have changed: the complexity of the management of diseases, the posion of physicians as only one more cog in the com-
plex machinery of medicine, the instuonal framework through which medical care is delivered. But mainly no longer is the
society in which the physician funcons what it was. There is no doubt that the current environment (and its values) are
more egocentric, more hedonisc, less community oriented and denitely more dedicated to the self. Polical leaders, ordi-
nary individual and mainly mass media exalt and promote rugged individualism and even demean social acon. In that con-
text, taking risks for social benet does not feel a “natural virtue” and make dicult to claim that the virtues remain un-
changed. Acknowledging that the virtues depend on context and are not immutable is what makes Arras suggest the emer-
gence of a historically determined model of the virtuous physician and why he asserts that virtues are "fragile". In a society
that does not call for high standards of virtues as empathy, solidarity and privileging the social good (and does not reward
those who pracce them) in many other essenal pracces, it may be dicult to ask only the HCWs to behave in such a vir-
tuous way.
Addionally, this duty even virtue-oriented must have limits. A disnct problem is to determine the threshold of “acceptable
risk,” the dividing line between duty and supererogaon. Some hazards clearly fall beyond the ambit of the doctor’s duty to
treat, but physicians should never be expected to subject themselves to blatantly suicidal risks or to go out of their way to
confront danger. Some extremely courageous acts may be deemed to be highly praiseworthy, but no one should induce doc-
tors to behave in that manner and much less blame a physician for not exposing him or herself to such high levels of risk.
While dening acceptable risk in the line of duty may be ambiguous amongst healthcare workers, moral dilemmas also arise
for those who feel their obligaons as healthcare professionals conicted with their obligaons to others as family members
and caregivers. Exalng altruism and heroism have the risk of forgeng that the rst duty of a physician during a pandemic
is to stay alive and that their delay of treatment to paents in order to take the me to suit up and protect themselves, is not
only jusable but necessary. Idencaon of duty to care with altruism makes invisible moral conicts between the vari-
ous pares to whom a person may owe care, and interferes with the need of healthcare professionals to understand and
accept that they must take all possible measures consistent with the social need for a funconing healthcare system to pro-
tect themselves in an epidemic. Duty to care should not be understood as the obligaon to noble self-sacrice. Physicians
have dues not only to current and future paents but to themselves as well as their families, colleagues, community and
society.

Humanitarian News
W A B I P N E W S L E T T E R P A G E 13
The processes of planning for pandemic inuenza, must include ethical discussion and must be carried out in advance. Oth-
erwise, there is a risk of making unjust and indefensible decisions aecng thousands of people. Physicians have to be pro-
tected, as well. They have the same rights as every human being and the duty of the government, policy makers and public
in general is to protect them as they are asking them for such exceponal behavior.
Finally, as a professional community we should understand that virtues and superogatory acts are ideals and aspiraons.
And it means that struggle and failure are compable with full possession of virtues and aspiraons. The possession of a vir-
tue or an aspiraon does not require its achievement or enactment on every occasion. Virtues are disposions revealed in
paerns of behaviour over me. We do not have the right to judge whether a person is courageous enough from a single
performance. Physicians who avoid caring for a risky paent but who in their other behaviour reveal their altruisc nature
should not be judged to lack this virtue.
This discussion should cover a multude of subjects. We cannot be blind at the fact that many doctors are already saying,
that they do not share the tradional vision of the good and that the current culture push physicians to the idea of medicine
as a career and not as a potenally self-sacricial vocaon. If some kind of opposion to the tradional duty grows up in the
medical profession, it could eventually undermine the claim that a professional duty sll exists.
Teaching dierently, specifying the limits of the duty of care, wring unambiguous codes, asking for a full understanding of
the sort of commitment required at the moment of entering the profession or creang clear contracts by which dierent
doctors may take dierent levels of commitment and receive dierent benets according to that , have all been proposed as
potenal soluons.
There is no doubt that this issue requires urgent aenon from researchers, regulatory bodies, and the public. And that if
civil society expects a high level of engagement and a special status of morality from the medical community, it will only be
possible if the medical profession regain its presge and independence and if during periods of crisis a more basic and uni-
versal social contract emerges. That broader social contract underlying the duty to care claims for the general public to per-
form his side of the contract in their role of supporng the healthcare system, to take responsibility of turning their work-
places as ‘safe enough’ under the circumstances; in adhering the recommendaons for protecng themselves and their
neighbours and in expressing their sincere support of the health care workers in concrete and human ways. Public must un-
derstand that in not doing that, they violate what ought to be a shared commitment to enacng a social value. This pandem-
ic (that for sure will not be the last one) highlights the need for calling for a broader social pact. If the society expects an al-
truisc behavior from HCWs and a health care system with the ability and the resources to give adequate answers during an
emergency, their members should crically reect about which moral values want to promote in the society and they must
promote and support egalitarian access to a strong health care system where the duty of care of the whole system sets the
general welfare above nancial prot or scal restraints.
References:
1. Singer P et al. BMJ. 2003; 327:1342–4.
2. Zuger A et al. JAMA. 1987; 258(14):1924-1928
3. Fox DM. The Polics of Physicians' Responsibility in Epi-
demics: A Note on History. Hasngs Center Report 1988, 18:
5-10
4. Daniels N. Duty to treat or Right to refuse. Hasngs Cen-
ter Report. 1991; 21(2): 36–46.
5. Malm H et al. Am J Bioeth 2008; 8:4-19
6. Pellegrino ED et al. New York: Oxford University Press,
1993:42–44
7. Tomlinson T. Journal of Medical Ethics. 2008;34:458-462
8. Bailey T et al. Am J Bioeth 2008; 8: 29-31
9. Reid L. Bioethics 2005; 19(4):348-61
*The views expressed in this arcle are those of the author (Silvia Quadrelli) and do not necessarily reect the ocial posi-
ons of the Execuve Board or Internaonal Board of Regents of the WABIP.
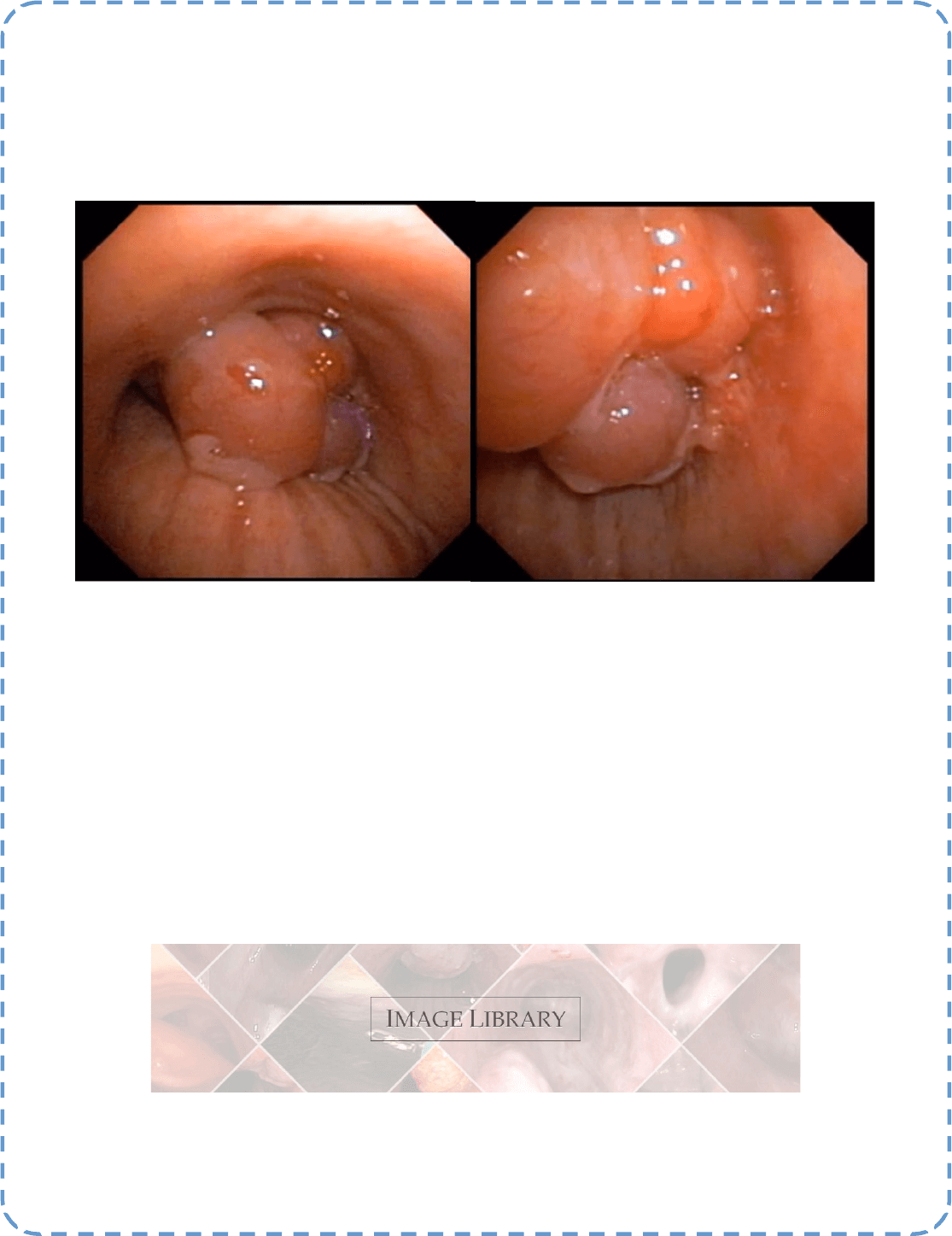
Best Image Contest 2020 Recipient (3 of 3)
Descripon: A polypoid lesion on the right lower tracheal wall ocluding almost completely the airway. The
lesion was resected with polipectomy snare and pathology revealed a WHO Type A thymoma. The paent, an
87-year-old woman, had been submited to surgical resecon of thymoma eleven years early.
Submiers: Liu Estradioto, MD and Rodrigo Beega de Araújo, MD.
*****
This image is 1 of 3 selected among 100+ submissions to our Best Image Contest held in 2019. Please stay tuned to the next Image
Contest, opening later this year!
Find the above image and more at the WABIP Academy Image Library!
Best Image Contest
P A G E 14
In Memory of Jean-François DUMON, M.D. (1939 - 2020)
It is with an extreme sadness, we have been informed that one of the fathers of intervenonal bronchoscopy, Dr. Jean-
François DUMON, passed away on July 14. 2020.
In such circumstances, it is common to draw the panegyric of the person, and even more when dealing with a promi-
nent medical leader and senior gure. It seems to be inappropriate for Jean-François DUMON because of the universal-
ly known link between his name and silicone stents. He was a strong advocate of intervenonal bronchoscopy through
rigid bronchoscopy and endobronchial laser.
He was in parcular a visionary for the use of silicone stents to manage endobronchial stenosis or obstrucon, based
on a strong daily clinical experience, demonstrang several decades ago, against the medical community at the begin-
ning, that this medical device was totally safe and useful for the paents. Jean-François DUMON has brought a revolu-
on in the management of central airway diseases and, in addion, was a dynamic leader both for the naonal and
internaonal organizaons dedicated to intervenonal bronchoscopy as well as for research in this eld. For his work
he has received numerous internaonal awards, among them the Killian Award of the WABIP being the most presg-
ious.
The internaonal pulmonology community has lost an instrumental leader and for several people, in parcular in our
area, a mentor and, humbly, a friend. His footsteps are heavily printed, and may his legacy be to a blessing for the next
generaons of intervenonal pulmonologists and for all the paents waing for new developments.
Our thoughts, these days, go to his family who stood by his side throughout his whole career, and to all the numerous
pulmonologists who have been trained or have aended courses in his “laser center” at Sainte Marguerite Hospital,
Marseille, to modestly catch a bit of his knowledge in rigid bronchoscopy, laser, and airway stenng.
Philippe ASTOUL, MD, PhD
Hervé DUTAU, MD
Department of Thoracic Oncology, Pleural Diseases and Intervenonal Pulmonology - Hôpital NORD – Marseille -
France
WABIP NEWS
P A G E 15

WABIP Awards Recipients 2020 -- We are very pleased to announce the recipients of the 2020 WABIP Awards. Our as-
sociaon humbly recognizes the below persons for their achievements and clinical pracces that have long made signicant
impact on the art and science of bronchology and intervenonal pulmonology:
Descripons of the Awards may be found at hps://www.wabip.com/awards
The WABIP Awards are presented bi-annually at our WCBIP. As our coming congress will be held virtually this year, presenta-
ons will also be in the same format. We will announce further details via social media and email. Stay tuned!
WCBIP Congress 2020 goes virtual only -- Due to local re-
stricons in Shanghai, our November 19-22 congress will be a virtu-
al-only event in which we will oer both live streaming and pre-
recorded lectures.
We are very excited to move forward with many lecturers around
the world contribung to our scienc program. Lectures will in-
clude topics ranging from EBUS TBNA, Cryobiopsy, Navigaonal bronchoscopy, bronchoscopic treatment of obstrucve lung
disease (emphysema, bronchis, asthma, Pediatric IP and much more!
Registraon fees have been reduced to $49 for WABIP members, and $69 for non-WABIP members. Further details of the
program, format, faculty and more at hp://www.WCBIP.org
We look forward to your parcipaon in our WCBIP Shanghai Virtual this November.
WABIP NEWS
P A G E 16
The Gustav Killian Centenary Medal
Recipient: Eric Edell, MD
The WABIP-Dumon Award
Recipient: Hervé Dutau, MD
The WABIP Lifeme Achievement Award
Recipient: Hugo Boo, MD
The Disnguished WABIP Regent Award
Recipient: Erik van der Heijden, MD

Tracheostomy in COVID-19 paents
Damned if I do, damned if I don’t
Like many procedures in medicine and surgery, tracheostomy has been reevaluated in the backdrop o COVID-19 Pandemic. Air-
way procedures such as tracheostomy and bronchoscopy expose proceduralists and the ancillary sta present in the room to a
much higher risk of airborne infecons than non-airway procedures. However, tracheostomy’s ambiguity of indicaons and urgent
nature should make us pause and think about this procedure's necessity and safety in these unprecedented mes.
It is imperave to understand the balance between the need and the risk of performing a tracheostomy in paents with COVID 19
and venlator-dependent respiratory failure. A concerted eort by CHEST led to the publicaon of a consensus statement (1) to
provide a guide on the issues of preparaon, ming, and technique of tracheostomy in COVID 19 paents while minimizing the risk
of infecon to health care workers (HCW).
I have extracted the following points from the expert panel report with a clear understanding that this is a uid document that was
put together with limited experience and informaon on COVID 19. Our knowledge of how the COVID 19 spreads and impacts ex-
tremely variable hosts due to comorbidies and inherent biological variability are rapidly evolving. I am condent that this docu-
ment will connue to morph as we gain more knowledge and experience in COVID 19.
The expert panel suggested that:
1. Tracheostomy be considered in coronavirus disease 2019 (COVID-19) paents when prolonged mechanical venlaon is anc-
ipated (Strong Consensus).
2. There is insucient evidence for recommending a specic ming for tracheostomy in COVID-19 related respiratory fail-
ure (Consensus).
3. In paents with COVID-19 related respiratory failure, either open surgical tracheostomy (OST) or percutaneous dilataonal
tracheostomy (PDT) can be performed in paents expected to require prolonged mechanical venlaon (Strong Consensus).
Remarks: Ulizaon of techniques which minimize aerosolizaon is recommended when performing tracheostomy (Strong Consen-
sus).
Editor-in-Chief: Dr. Kazuhiro Yasufuku
Research
Primary Business Address:
Kazuhiro Yasufuku, Editor-in-Chief
WABIP Newsleer
c/o Judy McConnell
200 Elizabeth St, 9N-957
Toronto, ON M5G 2C4 Canada
E-mail: newsleer@wabip.com
P A G E 17
Associate editor:
Dr. Ali Musani
Associate editor:
Dr. Sepmiu Murgu

P A G E 18
4. Enhanced personal protecve equipment (PPE) be used to migate the risk of health care worker related infecon during tra-
cheostomy (Strong Consensus).
Remarks: Tracheostomy is an aerosol generang procedure (AGP) and poses an infecon risk to HCW involved in the procedure
(Strong Consensus).
5. In paents with COVID-19 related respiratory failure, tracheostomy is performed in a negave-pressure room, preferably in
the ICU. As an alternave, a negave-pressure room in the OR could be used, with special aenon to minimizing transportaon
-related risk of exposure (Strong Consensus).
Remarks: If negave pressure rooms are unavailable, the procedure could be performed in a normal pressure room equipped with
HEPA lters in the presence of a strict door policy (Strong Consensus).
6. Roune RT-PCR tesng (nasopharyngeal swab or lower respiratory sample) prior to performing tracheostomy in paents with
conrmed COVID-19 related respiratory failure is NOT needed (Strong Consensus).
Remarks: There is insucient evidence to recommend RT-PCR tesng in paents with non-COVID-19 respiratory failure prior to
tracheostomy. If such tesng is performed, we suggest that a lower respiratory sample (endotracheal aspirate) rather than a naso-
pharyngeal swab be obtained (Consensus).
7. In paents with COVID-19 related respiratory failure, tracheostomy is performed by a team consisng of the least number of
providers with the highest level of experience (Strong Consensus).
Remarks: Authors suggest that prior to the iniaon of tracheostomy, a muldisciplinary group of providers including the primary
crical care team, palliave care, infecous disease, the procedural and airway team ulize respecve experse to determine the
goals of care, paent selecon, procedural consideraons, as well as workow to opmize safety of both paent and HCW (Strong
Consensus).
8. Paents be maintained with a closed circuit while on mechanical venlaon with a tracheostomy tube and with in-line suc-
on (Strong Consensus).
An extensive detail regarding the raonale and the references behind each recommendaon menoned above can be found in the
original statement. I strongly recommend anyone doing tracheostomy to review this statement. Be safe!
Reference:
1. Carla Lamb et al: Chest. 2020 Jun 6. doi: 10.1016/j.chest.2020.05.571
P A G E
19
WABIP ACADEMY- WEBCASTS
The WABIP has started a new educaon project recently: THE WABIP ACADEMY. The WABIP Academy will pro-
vide free online webcasts with new and hot topics that will interest pulmonologists and intervenonalists.
Current webcast topic: Tissue acquision for biomarker directed therapy of NSCLC
You can reach these webcasts by using this link: hp://www.wabipacademy.com/webcast/
www.bronchology.com Home of the Journal of Bronchology
www.bronchoscopy.org Internaonal educaonal website for
bronchoscopy training with u-tube and
facebook interfaces, numerous teachiing
videos, and step by step tesng and assess
ment tools
www.aabronchology.org American Associaon for Bronchology and I
ntervenonal Pulmonology (AABIP)
www.eabip.org European Associaon for Bronchology and
Intervenonal Pulmonology
W A B I P N E W S L E T T E R
Links
www.chestnet.org Intervenonal Chest/Diagnosc Procedures (IC/DP)
NetWork
www.thoracic.org American Thoracic Society
www.ctsnet.org The leading online resource of educaonal and
scienc research informaon for cardiothoracic
surgeons.
www.jrs.or.jp The Japanese Respirology Society
sites.google.com/site/asendoscopiarespiratoria/
Asociación Sudamericana de Endoscopía Respiratoria
P A G E 19