Volume 08
Issue 02
May 2020
Inside This Issue
Opinion/Editorial, 2-3
Technology Corner, 4-6
Tips from the Experts, 7-9
Humanitarian News, 10-14
Best Image Contest, 15
WABIP News & Upcoming Events, 16
Research, 17-18
Links, 19
Bronchoscopy in Paents with Suspected or Conrmed COVID-19 Infecon
Guest Opinion/Editorial
WABIP Newsletter
M A Y 2 0 2 0 V O L U M E 8 , I S S U E 2
EXECUTIVE BOARD
Silvia Quadrelli MD
Buenos Aires,
Argenna, Chair
Hideo Saka MD
Nagoya, Japan,
Vice-Chair
Zsolt Papai MD
Székesfehérvár,
Hungary, Immediate
Past-Chair
David Fielding MD
Brisbane Australia,
Treasurer
Naofumi Shinagawa,
MD
Secretary General
Hokkaido, Japan
Guangfa Wang MD
Beijing, China,
President WCBIP 2020
Philip Astoul, MD
Marseille, France,
President WCBIP 2022
STAFF
Michael Mendoza
General Manager
Judy McConnell
Administrator
Kazuhiro Yasufuku
Newsleer Editor-in-
chief
P A G E 2
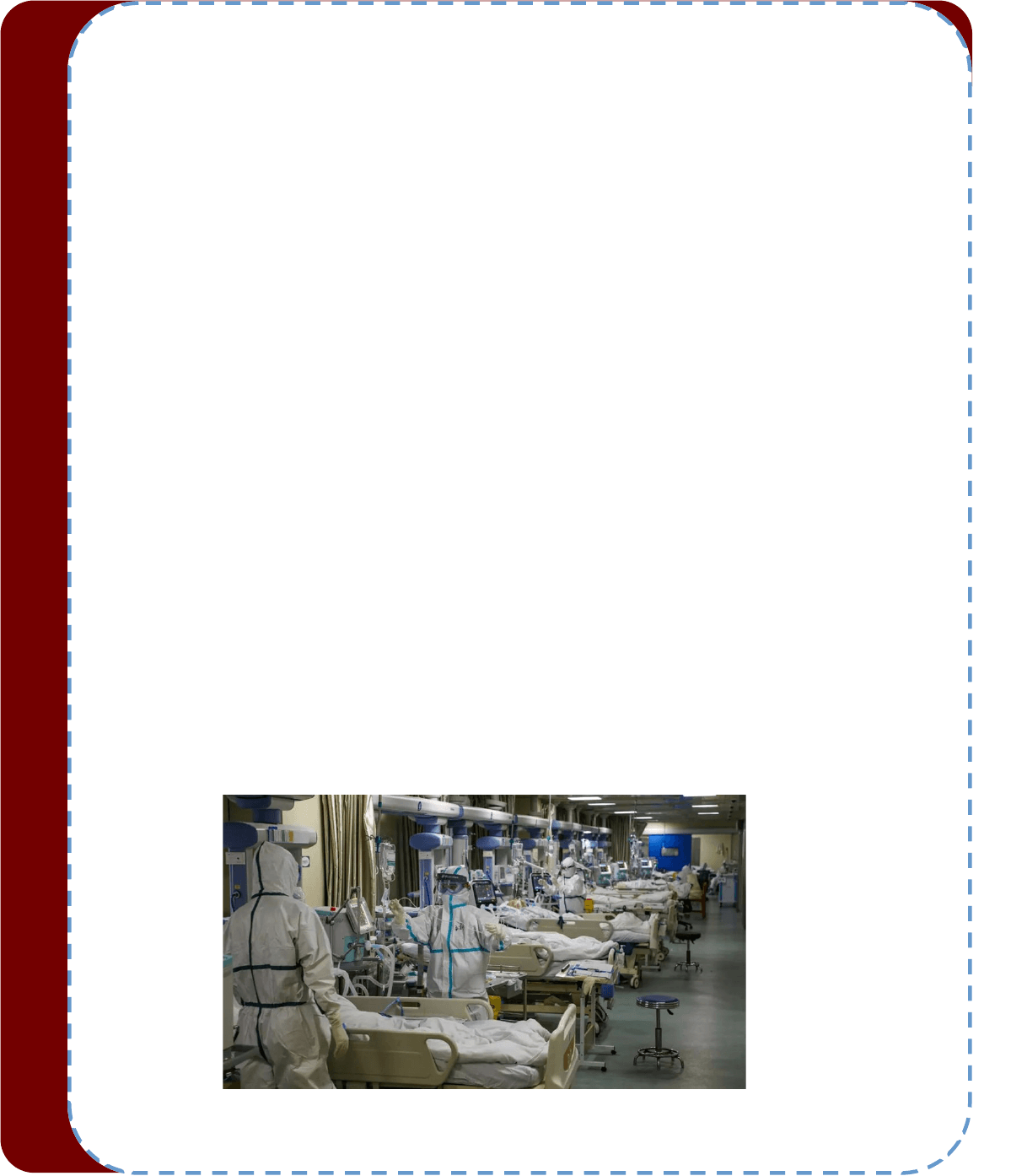
It has been more than 3 months since WHO was noed of the rst cases of “pneumonia with unknown cause” in
China. It’s incredible to reect on how dramacally the world has changed in such a short period. The total num-
ber of COVID-19 cases has passed three million, and the deaths related to COVID-19 is growing upwards of 217
thousand. No geographic region is spared from this pandemic. According to the latest WHO reports, the COVID-19
pandemic is spreading and taking grip in Africa aer Asia, Europe, and America. The devastang eects of COVID-
19 pandemic on human health, economy, and the social fabric of our global community will not be fully evident
for years to come. Unl then, extreme prevenons, necessary infecon control measures, and following expert
advice from the professionals will be the most prudent approach. No one country can combat this global pandem-
ic individually. Our approach to this highly fatal and devastang illness has to be global. Organizaons like WABIP
can genuinely play a global role in guiding its members around the world on how best to handle dicult issues of
performing necessary bronchoscopies and airway procedures vs. postponing them during this crisis. We can pro-
vide leadership to our members on how best to balance providing service to our fellow cizens and preserving
health care worker’s safety without feeling guilty or shame. We, the health care workers, are a nite resource for
the millions of very sick paents around the globe who need our help more than ever before. We need to be judi-
cious in ulizing this resource. Pulmonary and Crical Care Medicine is at the heart of the medical management
of COVID-19 paents. The vast majority of morbidity and mortality from COVID-19 stems from pulmonary prob-
lems.
Airway procedures, such as bronchoscopy, are being requested for reasons such as expedious diagnosis, man-
agement of complicaons, opmizing venlator management, and tracheostomy related to COVID -19 beside
roune indicaons. It is more important than ever to be extremely mindful and judicious in making decisions as to
the indicaons of these procedures. The risk and benets must be thoroughly weighed before embarking upon
any airway procedures in the backdrop of a highly contagious infecon that has no specic prophylacc or thera-
peuc opons. The implicaons of contaminaon of instruments and consequently infecng several people from
a straighorward procedure such a bronchoalveolar lavage could be devastang. These procedures could start a
cascade of eects jeopardizing the health of several health care workers and slow down the delivery of health
care to numerous other paents due to the consequent lack of health care workers and shortage of personal pro-
tecve equipment (PPE).
Below is the summary of guidelines provided by the American Associaon for Bronchology and Intervenonal
Pomology (AABIP) and the Society of Advance Bronchoscopists (SAB) in their recent consensus statements (1,2).
1. It’s preferable to collect upper respiratory samples via nasopharyngeal and oropharyngeal swabs for the diag-
nosis of COVID-19 at any stage of the disease.
2. Induced Sputum Collecon is NOT recommended.
3. Bronchoscopy carries a very high risk of aerosolizaon of the virus. Hence it has a very limited role in the diag-
nosis of COVID-19 infecon.
4. If an alternave diagnosis is suspected aer COVID-19 infecon has been ruled out, the paent should be intu-
bated for bronchoscopy to minimize the aerosolizaon of the virus and to expose the physicians and the sta.
This should only be done when there is a substanal change in management expected from new/alternave dis-
covery.
Ali I. Musani MD, FCCP
Vice Chair, Global Health. Department of Medicine
Professor of Medicine and Surgery
Director, Complex Airway Pillar of the Center for Lung and Breathing
Director, Bronchoscopy Service, Intervenonal Pulmonology Program and Fellowship
Division of Pulmonary Sciences & Crical Care Medicine
University of Colorado School of Medicine, Denver
5. Bronchoscopy should be performed in an Airborne Infecon Isolaon Room (AIIR ) negave pressure room.
6. Extreme care should be taken when collecng and handling specimens from paents who could be COVID-19 posive. Even the
paents who were COVID-19 negave a few days prior to the procedure, could be posive for COVID-19 at the me of bronchosco-
py. The current tests for COVID-19 are not 100% sensive or specic.
7. Laboratory personnel should be alerted that the specimen is from suspected COVID-19 paents.
8. The bronchoscopy sta and specimen handling sta should be limited to the minimum required personnel.
9. All personnel should wear a powered, air-purifying respirator (PAPR) or N95 mask and eye protecon.
10. All personnel should wear standard Personal Protecve Equipment (PPE), which includes gown, gloves, respiratory protecon,
and eye protecon.
11. Follow US Centers for Disease Control (CDC) instrucons for proper donning and dong of all protecve equipment and dispos-
able devices.
12. Disposable bronchoscopes should be used the rst line when available.
13. Follow standard disinfecon protocol of durable re-usable video monitors.
14. Follow standard high-level disinfecon for re-usable bronchoscopes.
15. Emergent bronchoscopy (same day) should be considered for the following condions: Acute foreign body aspiraon, massive
hemoptysis without obvious sources for embolizaon, and severe symptomac airway obstrucon.
16. Urgent bronchoscopy (1-2 days) should be considered in condions such as neutropenic fevers with pulmonary inltrates with-
out any other explanaon and lung transplant paents with clinical deterioraon despite empiric therapy.
17. The numbers of COVID-19 paents around the world are declining slowly but surely. Procedure lists have obtained a short but
robust experience in performing the invasive procedure with utmost care. Most centers are now performing lung cancer diagnosis
and staging with bronchoscopy as soon as possible. The urgency of diagnosis and staging of lung cancer has superseded the ultra-
conservave approach of delaying lung cancer diagnosis and staging. Bronchoscopy, for the diagnosis of recurrent or unresponsive
lung cancer, is also considered as an urgent procedure requiring early aenon. These decisions are best made under the auspices
of mul-disciplinary lung cancer teams.
18. Bronchoscopic procedures such as Bronchoscopic Lung Volume Reducon (BLVR), Bronchial Thermoplasty (BT), specimen col-
lecon for chronic infecons such as atypical mycobacterial and fungal infecons, and roune surveillance bronchoscopies for lung
transplant paents should be postponed unl the polices for such procedures have been developed, and the risk of COVID-19 is
signicantly lower.
19. Avoid rigid bronchoscopy, if possible, and if necessary, use without jet venlaon .
20. If a bronchoscopist or a bronchoscopy team member is exposed during the procedure, he/she should let the other bronchosco-
pist/team member nish the case (if safely possible). He/she should be tested if the source paent is conrmed as posive for
COVID-19. Return to work should follow the hospital and local polices around tesng, resoluon of symptoms, and permission
from a physician.
In conclusion, bronchoscopy should be avoided in the vast majority of paents with suspected or proven COVID-19 unless there
are emergent or urgent indicaons. If it must be performed, extreme precauons and safety measures should be taken by using
proper PPE and curtailing of aerosolizaon of the virus. The recommendaons for bronchoscopy and all other procedures are rap-
idly evolving with our understanding of transmission, virulence, possible therapies, and improving technologies for dealing with
COVID-19. The recommendaons may also vary depending upon the local burden of disease, resources, and experse. Please con-
nue to follow local and internaonal guidelines and expert reports.
References:
1. American Associaon for Bronchology and Intervenonal Pulmonology ( AABIP ) Statement on the Use of Bronchoscopy and Respiratory
Specimen Collecon in Paents with Suspected or Conrmed COVID-19 Infecon. Accepted for publicaon in journal of Bronchology. aabron-
chology.org
2. J Thorac Dis 2020 | hp://dx.doi.org/10.21037/jtd.2020.04.32
W A B I P N E W S L E T T E R
P A G E 3
Technology Corner
Trans-parenchymal nodule access
INTRODUCTION
During the past decade, there has been a remarkable advancement in diagnosc technological innovaons with respect to bron-
choscopic approaches of an indeterminate pulmonary nodule. These include: ultrathin bronchoscopy, radial endobronchial ultra-
sound (rEBUS), virtual bronchoscopy, electromagnec navigaon bronchoscopy, roboc bronchoscopy as well as combinaons of
these techniques. The diagnosc yield of such technologies is usually dependent on several factors such as size of the pulmonary
nodule, anatomical locaon, airway bronchus sign, eccentric or concentric view on rEBUS and CT-to-body divergence during bron-
choscopy. Furthermore, airway anatomy is complex making navigaon and maneuvering through several subsegments very chal-
lenging leading to probably lower yield beyond fourth-generaon bronchial segments.
BACKGROUND
One of the limitaons of the above technologies is the challenge of accessing a lung nodule without a bronchus sign on CT chest.
Two novel bronchoscopic techniques, bronchoscopic trans-parenchymal nodule access (BTPNA) and transbronchial access tool
(TBAT), have been developed that allows bronchoscopists to overcome such limitaon by accessing nodules through an airway wall
independent of an airway leading to the lesion.
BTPNA
The Archimedes Virtual Bronchoscopy Navigaon System (Broncus Medical, Mountain View, California, USA) (Figure 1) recon-
structs pre-procedural CT scan into a 3D model which provides guidance of a sheath from the point of entry on the airway wall
through the lung parenchyma directly to the lung nodule using a balloon catheter equipped guided sheath. The point of exit to the
airway wall can be computer selected or adjusted per physician preference. The vasculature is highlighted with a “virtual Doppler”
funcon to help avoid vessels at the exit point. During the procedure, airway wall is punctured with a 18G needle followed by di-
lang the hole with a balloon then advancing the guide sheath with blunt stylet (steerable catheter) through parenchymal ssue
into the nodule under real-me uoroscopy. There is a fusion of the virtual plan from CT data with the real-me uoroscopy image
where the passage of the sheath can be corrected real me.
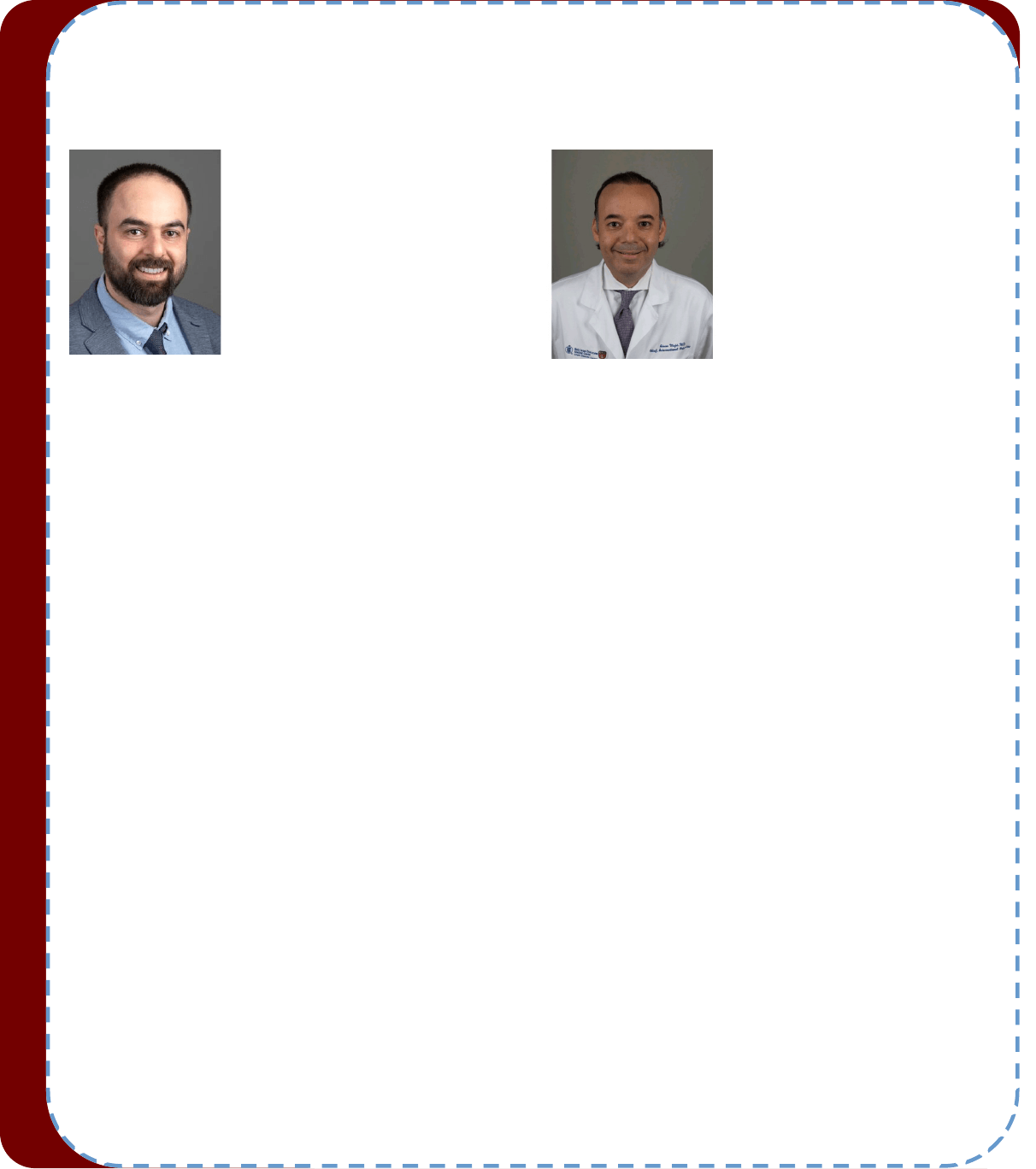
TBAT
The CrossCountry
TM
TBAT (Transbronchial Access Tool) (Medtronic, Minneapolis, Minnesota, USA) (Figure 2) has been also de-
signed to allow access through an airway wall and into the lung parenchyma for lesions without an airway. Once the opmal air-
way exit point is planned, constructed from pre-procedural CT data and reached during the electromagnec navigaon bronchos-
copy, a small sharp pped wire is deployed through the airway wall and into the parenchyma. Then, a cone-shaped dilator is
W A B I P N E W S L E T T E R
P A G E 4
Adnan Majid, MD
Division of Thoracic Surgery and
Intervenonal Pulmonology, Beth
Israel Deaconess Medical Center,
Harvard Medical School, Boston, MA
Fayez Kheir, MD MSc
Division of Thoracic Surgery and
Intervenonal Pulmonology, Beth
Israel Deaconess Medical Center,
Harvard Medical School, Boston, MA

advanced over the wire, through the airway wall and into the parenchyma to the lung nodule. Using Seldinger technique, the extended
working channel/Edge
TM
catheter is advanced over the dilator while pulling the wire back. The catheter is directed over the central dilator
unl the proximal end of the lung nodule is reached. The wire and dilator are then removed leaving access for biopsy tools though the ex-
tended working channel/Edge
TM
catheter under uoroscopy.
CLINICAL APPLICATION
Clinical data regarding BTPNA is sll emerging. The rst-in-human report was published by Herth et al. in 2015. 10 out of 12 paents with
suspicious lung nodules were successfully accessed using Archimedes Virtual Bronchoscopy Navigaon System in combinaon with com-
puter-enhanced fused uoroscopy transparenchymal access followed immediately by surgical resecon. Adequate biopsies were obtained
from the 10 paents (83%), which correlated with the histological ndings from the surgical resecon.
1
There were no peri or post-
operave complicaons aside from a transient elevaon of troponin in one paent. Inspecon of the resected lobes showed no hemor-
rhage or parenchymal laceraons. Another small study performed in a bronchoscopy suite showed that successful BTPNA and adequate
biopsy was obtained in 5 out of 6. Pneumothorax was reported in 2 of the 5 paents (one required chest tube) and no other adverse events
were reported.
2
A large mulcenter trial including 6 U.S., 1 Germany and 3 China ses, Evaluaon of the Archimedes™ System for Transpar-
enchymal Nodule Access 2 (EAST2) (NCT02867371), was recently completed with data presented in the recent ERS Congress.
3
A total of 106
paents were enrolled in the study and the results will hopefully provide further data on the technique’s safety and diagnosc yield.
There is sll paucity of literature regarding TBAT. Two small case series have been published on the safety and feasibility of such device.
Anciano et al. described three cases using TBAT.
4
Although the nodule was successfully reached in all three cases, only 2 had denive diag-
nosis. There were no adverse events reported. Another small case series by Bowling et al. used a combinaon of cone beam computed to-
mography scan, electromagnec navigaon and TBAT.
5
9 out of 12 lung nodules/masses (75%) were successfully accessed with TBAT with a
diagnosc yield of 66% (8 of 12). One paent had a pneumothorax and required a chest tube.
Furthermore, about a third of paents with potenally curable disease do not undergo surgical resecon due to dierent reasons such as
advanced lung disease, medical comorbidies or age. Trans-parenchymal nodule access may facilitate local treatment of early lung cancers
in such paent populaon.
CONCLUSION
Numerous advanced bronchoscopic techniques have occurred in the pursuit of improved diagnosc yield for peripheral pulmonary nod-
ules. The ability to safely access lung nodules located away from the bronchial airway for diagnosc and eventually therapeuc modality is
appealing. However, high-quality mulcenter trials to validate diagnosc yield and safety results as well as comparing such technique
against transthoracic or even among dierent modalies of transbronchial lung biopsies are needed.
References:
1. Herth FJ et al. Thorax 2015; 70:326-32
2. Harzheim D et al. Respiraon 2016; 91:302-6
3. European Respiratory Journal 2019; 54: Suppl. 63, OA1614
4. Anciano C et al. J Bronchology Interv Pulmonol 2017; 24:253-6
5. Bowling MR et al. Ann Thorac Surg 2017; 104:443-9
W A B I P N E W S L E T T E R P A G E 5
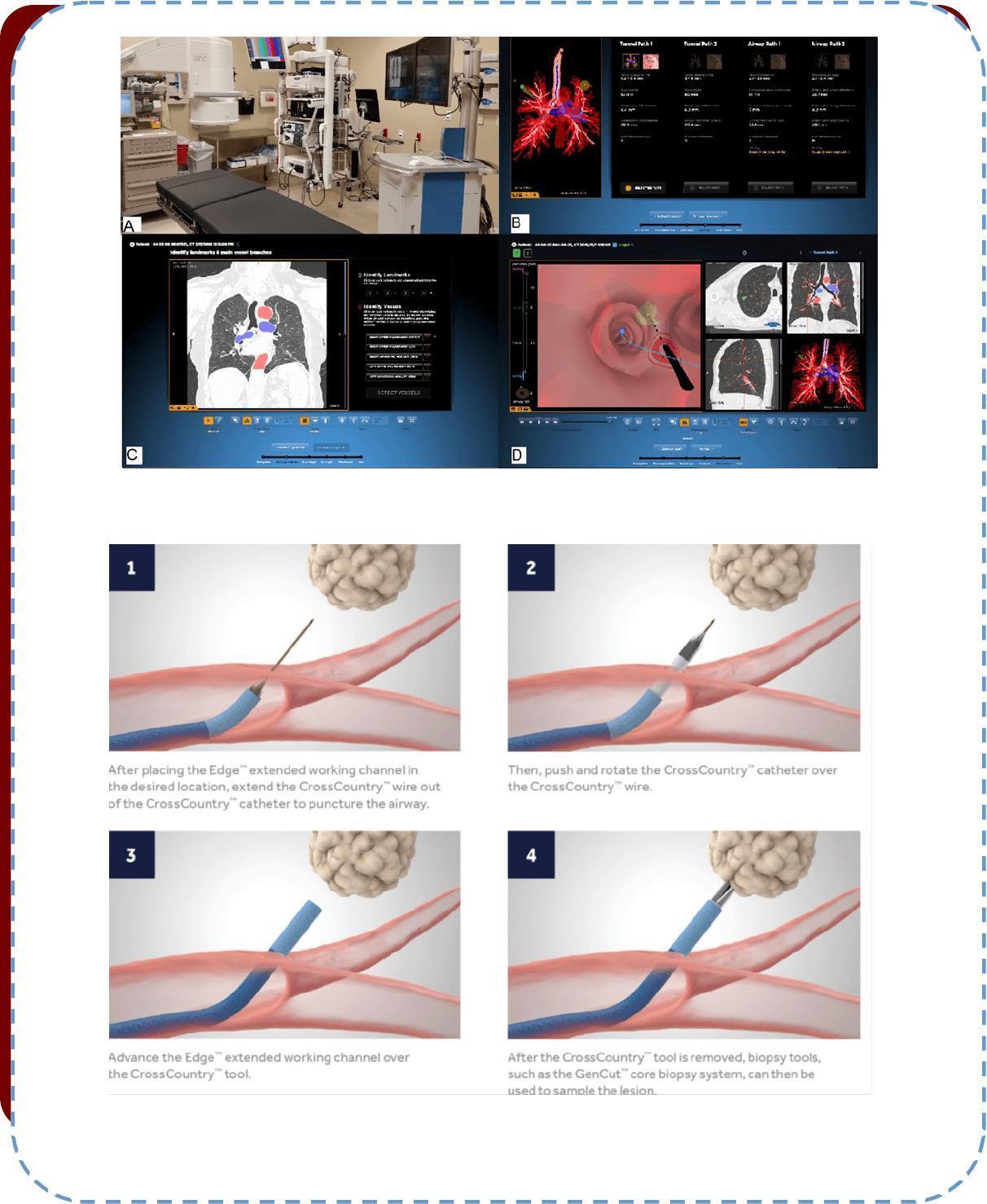
Figure 1: A. Procedure room, B. Selecng path image, C. Idenfying vessels, D. Selecng point of exit (Images courtesy of Broncus Medical)
Figure 2. Crosscountry transbronchial access tool (Images courtesy of Medtronic)
W A B I P N E W S L E T T E R P A G E 6

Tips from the Experts
P A G E 7
V O L U M E 8 , I S S U E
Introducon
Lung cancer screening and the increased use of chest computed tomography (CT) has led to a signicantly high rate of lung nodules detec-
on. In the United States, 1.6 million nodules are predicted to be detected every year. The limitaons of currently available convenonal
and guided bronchoscopy plaorms for diagnosing peripheral lung nodules have led to the introducon of robot assisted bronchoscopy.
This technology allows the bronchoscopists to navigate through small airways under direct visualizaon and EMN guidance. Two roboc
systems have been commercially available for almost 2 years and have shown promising results in cadaveric models in regards to further
reach to the periphery compared to convenonal bronchoscopy. A recent retrospecve post post-markeng mulcenter study using the
Monarch
TM
Auris roboc plaorm in 165 paents showed successful navigaon (dened as acquision of a r-EBUS image or diagnosc s-
sue) to 88.6% of the lung nodules. In this study, the maximum diagnosc yield was esmated at 77% and the majority (70.7%) of the nod-
ules were located in the outer third of the lung. From this experience, we learned several planning and technical ps that we believe could
lead to improved access and diagnosc yield.
Planning
Prior to each case, we carefully review the CT scan and idenfy the airways in the proximity of the lesion. If there is no airway directly lead-
ing to the lesion (lack of the “bronchus sign”), we follow the blood vessel adjacent or leading to it, based on the understanding of pulmonary
segmental anatomy. This assumes that lesions without a “bronchus sign” with a vessel leading to them have an adjoining airway, even if not
seen on the CT scan (as it’s oen the case in paents with emphysema). We also always create our own manual path using the system’s
soware and do not only rely on the automac planning. In addion, we write a “mental pathway” (scope orientaon at each branching
point).
A standard room set up is used with a dedicated team who received prior training. We ensure removal of any large metallic objects from the
operang table and surrounding the EM eld generator during the set up and EM navigaon phase of the procedure. We use general anes-
thesia with an 8.5 endotracheal tube. An airway inspecon is performed prior to the procedure to assess for endobronchial lesions and ther-
apeuc aspiraon of secreons. Once that is completed, the roboc bronchoscope is loaded and advanced to the trachea. Registraon is
completed by touching the carina and advancing the bronchoscope into the contralateral mainstem bronchus. This is a smooth, unrushed
process while avoiding airway wall trauma. Unless precluded by the underlying disease, dal volumes of 6-8 ml/kg and PEEP levels of 8-15
are used to splint open the distal airways. These sengs are applied prior to wedging the roboc bronchoscope sheath in a segmental air-
way. The bronchoscope and the sheath are advanced as a unit into the target segmental or even sub-segmental airway. This helps wedge
the scope and protect ipsilateral lobes or contralateral lung in case of bleeding. The inner bronchoscope is then advanced to the target seg-
ments based on virtual guidance from the EMN system or based on the operator’s own “mental plan”. While the RAB systems allow for an
enhanced reach in the lung periphery, on occasion the small airway may not be visualized due to their collapsibility (as is the case in paents
with severe emphysema). This can be overcome by allowing pressure equilibraon between the target airway and the atmosphere by transi-
ently disconnecng the proximal valve of the working channel. If this is not successful, the scope can be relaxed (it takes a co-axial posion)
and air can be insuated through the working channel using a 60 ml syringe allowing for transient splinng of the small airways. While the
airways are opening up with gentle air insuaon, the scope is advanced to the next generaon airway. Occasionally, we use a closed for-
ceps tool as a guidewire to enter increasingly smaller peripheral airways.
Tips for improving the navigaon, visualizaon and specimen quality during
Roboc Assisted Bronchoscopy
Sepmiu Murgu MD, FCCP, DAABIP
University of Chicago
Abhinav Agrawal MD
University of Chicago
P A G E 8
V O L U M E 8 , I S S U E
Sampling
Once we reach the target based in EMN guidance, radial-EBUS (rEBUS) is always performed to conrm the target and to assess its relaon to
the bronchial wall (Figure). Once an acceptable rEBUS view is obtained (concentric or eccentric), the bronchoscope is locked in place, and we
start sampling using a transbronchial aspiraon needle to perform 4-5 passes under uoroscopic guidance. During sampling, in case an eccen-
tric rEBUS view is noted, the scope can be oriented towards the target airway as rEBUS can be used to idenfy the locaon of lesion as long
as peripheral visualizaon is maintained. Subsequently, the needle is advanced in the same direcon to puncture through the airway wall and
samples are obtained.
Rapid onsite cytology evaluaon is performed in all cases in our instuon, although the value of this pracce remains to be determined. The
Di Quik smeared needle specimens are reviewed by a pathologist. If an adequate representave specimen is conrmed, we ensure that
more adequate material is obtained for any ancillary tesng including molecular markers; this involves performing extra needle passes (our
molecular laboratory uses cytology smears for comprehensive molecular tesng) and then we proceed with transbronchial forceps biopsies.
If the needle aspiraon is non-diagnosc aer 4- 5 passes, then we use the Auris transbronchial biopsy forceps to perform 4-5 biopsies under
uoroscopic guidance. Touch preps are performed for rapid onsite cytopathology evaluaon. These samples are sent for further histopatho-
logic exam in 10% formalin soluon. Of note, we do not ush the needles with saline unless there is diculty reloading the stylet. If needles
are ushed with saline, then they should be subsequently ushed with air several mes unl the working channel is dried out. This is because
the presence of saline uid in the working channel could compromise the quality of the subsequent Di-Quik smear.
Quality control
Appropriate history and physical examinaon should be performed and the expected diagnosc yield, limitaons, as well as the risk and ben-
ets should be thoroughly discussed with the paent prior to proceeding with RAB. In paents with pacemakers or debrillators, the use of
the electromagnec eld generator may interfere with their funconing, and thus the use of an alternave technology of guided bronchosco-
py or other modalies for biopsy should be considered unl more data proves safety of RAB in this paent populaon.
A careful review of the chest CT scan prior to planning a roboc bronchoscopy is essenal to set up for a successful procedure. Apart from
idenfying the lesion and the adjacent airways, it is also essenal to assess for presence of possible endobronchial lesion, especially in the
distal airways leading to the target lesion. If an endobronchial lesion is noted, a thin exible bronchoscope can be used instead of a using the
expensive RAB scope and tools to achieve the diagnosis. Similarly, the CT and PET/CT should be assessed for mediasnal adenopathy. If nodal
enlargement or involvement is noted or expected, a linear EBUS may suce to provide diagnosis and staging with a lower risk of complica-
ons and precluding the roboc assisted bronchoscopy altogether. On the other hand, if suspicion of nodal involvement is low, the RAB
should be performed rst, before the EBUS-TBNA. This is because we are learning that aer approximately 20 mins of general anesthesia,
certain areas of the lung may become atelectac, making navigaon more dicult and potenally giving false posive rEBUS or cone beam
CT images.
The small roboc scope and a steady sheath provide the ability to navigate to distal airways, but in some paents with radiaon associated
brosis, COPD or tortuous airways, it might be dicult to navigate the roboc bronchoscope into the apical or posterior segments of the right
upper lobe. In these cases, the operator should acknowledge the limitaon, and if repeated aempts are unsuccessful, look for alternave
modalies to achieve the diagnosis rather that risk injury to the airway by persistent maneuvering. The use of saline, in addion to potenally
compromising the quality of the specimens, can also give false posive rEBUS image or cone beam CT images by causing alveolar lling. In
cases with poor airway visualizaon, air insuaon can be used to enhance the view as menoned above. Finally, a post-procedure radiog-
raphy should be performed at the end of the procedure to assess for any complicaons.
Conclusion
RAB oers improved access to the periphery of the lung and stability while working at the target. Aer 18 months of experience with this
technology, we learned several ps for improving planning, navigaon, peripheral airway visualizaon and specimen handling. We trust that
some of these technical aspects can be applied in future studies of RAB with the aim to further improve the inially reported diagnosc yield.
References
1. Gould, ML et al. AJRCCM. 2015;192:1208-14.
2. Murgu, S. BMC Pulmonary Medicine. 2019;19(1);89.
3. Chaddha U et al. BMC Pulmonary Medicine. 2019;19(1);243
4. Chen AC et al. Respiraon. 2020;99:56-61
5. Agrawal A et al. Journal of Thoracic Disease. 2020.
Tips from the Experts
P A G E 9
V O L U M E 8 , I S S U E
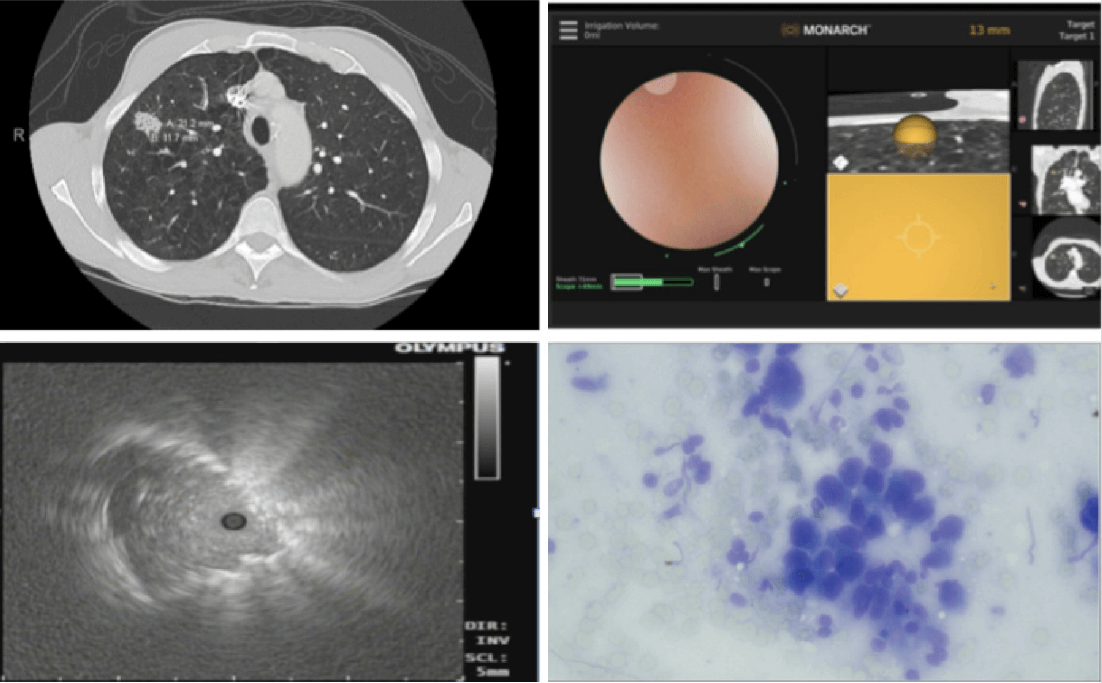
Figure 1. Roboc bronchoscopy for a 2.1 cm peripheral right upper lobe nodule. Top Le: CT Chest demonstrang a 2.1 cm right upper
lobe nodule. Top Right: Robot bronchoscopy using the Monarch Auris Roboc Assisted Bronchoscope with an endobronchial view and
electromagnec navigaon guidance showing the locaon of the nodule. Boom Le: Eccentric rEBUS view conrming the locaon of the
nodule. Boom Right: Di Quick stain demonstrang adenocarcinoma.
Tips from the Experts
Humanitarian News
W A B I P N E W S L E T T E R P A G E 10
ETHICS OF PUBLIC HEALTH DURING A PANDEMIC
Medicine and public health are two complementary and interacng approaches for promong and protecng health. Yet
medicine and public health can, and also must be dierenated, because in several important ways they are not the same.
The fundamental dierence involves the populaon emphasis of public health, which contrasts with the essenally individu-
al focus of medical care. Public health idenes and measures threats to the health of populaons, develops governmental
policies in response to these concerns, and seeks to assure certain health and related services. In contrast, medical care fo-
cuses upon individuals-diagnosis, treatment, relief of suering and rehabilitaon.
In early bioethics, the good of the individual, and parcularly his or her autonomy, was the dominant theme, not populaon
health. The last two decades following infecous outbreaks and global health threats have produced a resurgence of visibil-
ity for public health. Addionally, it is becoming impossible to avoid the recognion that the health of populaons is a func-
on more of good public health measures and socioeconomic condions than of biomedical advances, a well-known concept
within the public health community, but that has been neglected by most outside the eld.
Populaons are constuted by diverse communies of heterogeneous beliefs and pracces. These may at mes come into
conict. Individual versus community rights and conicts within and between communies are the origin of ethical discus-
sions in public health pracce. Hence, public health ethics must recognize and be able to reason through issues relang to
social, polical and cultural contexts; the existence of compeng values and perspecves and perhaps, diverse and some-
mes conicng world views.
Along the years, public health, has struggled to dene and arculate its core values and the language and structure of its
ethics. Given its populaon focus, and its interest in the underlying condions upon which health is predicated it seems evi-
dent that its ethical framework must express fundamental values in societal terms.
In social development, ethical discussions show the ongoing debate on values and choices in which each individual compares
and reects on his own experience and thought in juxtaposion to experience and thought of others. It is important to re-
mind that the credibility and viability of a democrac sociees depend crically on the conduct of ethical debate both
amongst members of the public and between members of the public and decision-makers.
Obviously, ethics in public health cannot be divorced to the background values of the general society, and the parcular
communies, in which it will be carried out. It is not realisc to expect that health care could survive as some sort of sepa-
rate enclave enrely dierent of society values. Those values — both good and bad — will inevitably permeate health care.
However, this does not mean health care has to be merely a passive observer of what is happening in society.
A main concern about the possibility of dening a set of core ethical values in public health is that public health measures
can quickly become policized. Even when many mes polical controversy may be seen (and really becomes) and obstacle
to raonality, the governmental role of public health turns polics unavoidable and necessary. Polics is a necessary compo-
nent of public health, precisely in order to achieve public health policies and pracces.
But beyond any polical controversies and even in pluralisc and diverse sociees, some ethical foundaons should be a
common ground shared by the whole society and the polical leaders and those are the grounds of the respect of human
rights.
Jonathan Mann famously theorized that public health, ethics, and human rights are complementary elds movated by the
paramount value of human well-being. He felt that people could not be healthy if governments did not respect their rights
and dignity as well as engage in health policies guided by sound ethical values. Nor could people have their rights and dignity
Humanitarian News
W A B I P N E W S L E T T E R P A G E 11
if they were not healthy, Mann and his colleagues argued that public health and human rights are integrally connected: Hu-
man rights violaons adversely aect the community’s health, coercive public health policies violate human rights, and ad-
vancement of human rights and public health reinforce one another.
Thus, in the modern world, public health ocials have, for the rst me, two fundamental responsibilies to the public: to
protect and promote public health, and to protect and promote human rights. Promong and protecng human rights is
inextricably linked with promong and protecng health, because human rights oers a societal-level framework for iden-
fying and responding to the underlying-societal—determinants of health. Human rights are respected not only for their in-
strumental value in contribung to public health goals but for themselves, as societal goods of pre-eminent importance. And
some of the most relevant founding basis of human rights are the respect for human dignity, solidarity and jusce and equi-
ty.
Mann, in both his naonal and internaonal work, conceived of human rights and ethics as centrally important to the work
of public health. Consequently, he passionately argued that the primary funcon of public health is to promote dignity, re-
duce inequity, and raise living standards for communies everywhere.
The Universal Declaraon of Human Rights starts by placing dignity rst, "all people are born equal in dignity and rights".
Some scholars have argued that dignity does not have a vocabulary, or taxonomy to dene dignity violaons. Some have
gone as far as declaring that dignity is a “useless concept”. However, we all know when our dignity is violated or impugned.
Dignity can be dened in several dierent, but complementary ways, which fall broadly into two categories: these are
‘inherent dignity’ and ‘non-inherent dignity’. Inherent dignity refers to a quality of value or worth belonging equally to every
human being; it is permanent, uncondional, indivisible and inviolable. Inherent dignity is related to, and oen used inter-
changeably with, the similar concept of ‘intrinsic value’ i.e. inviolable worth arising from within each person. Non-inherent
dignity (NID) is an acquired and variable condion; it is conngent upon a person’s circumstances and behaviour.
As Alasdair MacIntyre has pointed out, moral concepts are not meless or unchanging and so, the concept of dignity has
been used over me, in a variety of contexts with dierent meanings. But the concept of inherent dignity can be traced from
remote mes. A concepon of uncondional inherent dignity has been developed in both Chrisanity and Judaism. A theo-
logical understanding of dignity connues to be for some people based on the belief that humans are made in the image of
God and considered sucient to ground for the inviolability of human life.
This concept of dignity being connected to human nature is found in the Summa Theologiae by Aquinas and persisted during
the Renaissance period, when it began to be associated with freedom and autonomy.
However, there is no doubt that the most important development about dignity were the wrings of Immanuel Kant. Kant
argued that dignity is grounded in morality and autonomy. The Kanan concepon of dignity forms the foundaon of the
current understanding of inherent dignity used in much of human rights legislaon. Kant’s concepon of inherent dignity did
not depend on God in the tradional way, Kant laid the way for a secular understanding of inherent dignity. In his own words
“A raonal being belongs to the realm of ends as a member when he gives universal laws in it while also himself subject to
those laws. He belongs to it as sovereign when he, as legislang, is subject to the will of no other.”
Following publicaon of Darwin’s Origin of Species in 1859 some people quesoned assumpons about our species, and
under the inuence of Social Darwinism the unique inherent value of humans was rejected and even enabled the advance-
ment of the eld of eugenics. Aer the atrocies of WW2, an emphasis on dignity re-emerged in much of the internaonal
legislaon and the world returned to the concept of inherent dignity in declaring that all humans were inherently equal and
had intrinsic value, and thus that all human lives deserved protecon. Thus the United Naons in the UDHR (1948), states in
the preamble, ‘recognion of the inherent dignity and of the equal and inalienable rights of all members of the human family
Humanitarian News
W A B I P N E W S L E T T E R P A G E 12
is the foundaon of freedom, jusce and peace in the world”. Human dignity is now the most widely accepted fundamental
moral and legal value, appearing in the constuons of 157 countries, it is 81 per cent of the total number of sovereign
states of the UN.
“Full inherent dignity” is a quality of value or worth belonging equally to every being with full moral status and thus it is indi-
visible: there are not degrees of dignity, either a being has it or they do not; it cannot be had in part. Full inherent dignity is
both a permanent and uncondional quality.
The fundamental premise to the concept of full inherent human dignity is that it is innate to all human beings; in this regard
it can be thought to amount to (at least part of) what it is to be human. It implies that human dignity comes from belonging
to a natural kind, whose members have full moral status, such as humankind and determines the requirement that one be
treated with deference and respect, irrespecve of circumstances, no maer his age, race, sex, cognive autonomy, contri-
buon to society or the well-being of others. Each life is unique and irreplaceable, human beings should be treated as an end
in themselves and not as a means to something else. Just because they are human they value in itself and their inherent val-
ue does not depend on anything else, that is the foundaon of the Kanan imperave “Act in such a way that you treat hu-
manity, whether in your own person or in the person of another, always at the same me as an end and never simply as a
means”. Therefore, inherent human dignity has normave implicaons grounding fundamental human rights, such as the
rights to freedom and equality, and the right to live free from cruel and degrading treatment.
The Italian philosopher Corrado Viafora has advocated for the incorporaon of human dignity in ethically driven clinical case
management and some scholars have applied his concepts to public health. According to Viafora “In dealing with issues of
commutave and distribuve jusce, clinical ethics extends beyond its specic competence and steps, respecvely, into the
eld of polics and in the eld of law.” The recognion of “intrinsic value” based on the recognion of human dignity, is thus
the ulmate criterion for disnguishing amongst moral and immoral pracces.”
A reference to human dignity has been incorporated into the 1997 Oviedo Convenon of the Council of Europe and also into
the Charter of Fundamental Rights of the EU in 2000, establishing a common ethico-legal foundaon for all 28 sociees of
the EU Member States. According to Lucy Michael “(human) dignity maers, because it forms the foundaon of civilized soci-
ety.”
As such, human dignity understood in a public health ethical context should have the potenal to funcon as a common ba-
sis for jusfying legislave endeavors through ethical judgments in a pluralisc society, as being the value that fosters cultur-
al understanding to grant cizens a dignied life and above all to guarantee the uncondional worth of every human being.
But we human beings not only have dignity in common. In Dependent Raonal Animals, Alasdair MacIntyre remarks that the
philosophical tradion has neglected the importance of need or dependence as an aspect of human life. Especially since the
Enlightenment, the nature of human beings has been focused only on their freedom, raonality, or autonomy. But some
areas of philosophy (mainly but not exclusively amongst Chrisan thinkers) have always understood the human situaon as
one of dignity and dependence: a dignity that is common to all human beings but equally a neediness that is common to all.
While some individuals may think themselves independent and even self-made or self-sufcient, we are all dependent not
only physically but also culturally and intellectually, on a wider community and a longer tradion. All human beings are more
or less dependent on one another and accounts of human dignity should not seek to obscure this fact.
In the last two decades, several outbreaks of viral diseases that created a new global public health threat. It has been argued
there is an urgent necessity of intense and transnaonally coordinated preparaon of public health systems to combat those
pandemic threats. Consequently, transnaonal collaboraons are considered crucial to eecve exchange of genomic, clini-
cal, and epidemiologic data leading to the development of vaccines and treatment protocols and the idencaon of popu-
Humanitarian News
W A B I P N E W S L E T T E R P A G E 13
laon-based strategies. It is well known by experts in the epidemiological eld that a mely prevenve preparaon of
healthcare systems can be eecve in saving dozens of thousands of lives. Avoiding this “hidden death threat” is rst and
foremost a task of establishing a sustainable health prevenon policy that cares for its cizens on a populaon basis and on
grounds of human dignity, having as its rst and indeclinable objecve to protect the life of each individual cizen.
Somemes human beings can be morally responsible for the outcomes of not man-made disasters, blaming disgrace does
not erase such responsibility ascripons that will most oen be grounded in culpable negligence, including the culpable fail-
ure to prevent the side-eects of our acons or omissions. Denialism (as dened by Hoofnagle & Hoofnagle) is not a minor
component of these wrong policies. HIV does not cause AIDS, the world was created in 4004 BCE, smoking does not cause
cancer, there were no gas chambers in Auschwitz and climate change has nothing to do with man-made CO2 emissions.
The consequences of policies based on views such as these can be fatal. Thabo Mbeki’s denial that that HIV caused AIDS pre-
vented thousands of HIV posive mothers in South Africa from receiving an-retrovirals so that they, unnecessarily, trans-
mied the disease to their children. Denialism, dened as the employment of rhetorical arguments to give the appearance
of legimate debate where there is none, is driven by a range of movaons, from greed, lured by some big corporaons to
ideology or faith, causing them to reject anything incompable with their fundamental beliefs. Whichever the reasons, the
potenally fatal consequences of those atudes make people responsible of contribung to them or using them whichever
their purposes. The higher in the hierarchy of decisions about health care policies and decisions, the higher the responsibil-
ity.
The applicaon of general ethical principles to public health decisions can be dicult. The mandate of public health has been
prevenon, and the arena of public health pracce has been the community. In situaons when the enre community is
assumed to be vulnerable and in need of protecon, collecve intervenons are proposed which are mandatory, universal,
and passive, to minimize the risks. Public health disasters accelerate and accentuate the vulnerability dimensions of human
life.
Since the mission of public health is to achieve the greatest health benets for the greatest number of people, it draws from
the tradions of ulitarianism or consequenalism. The “public health model,” has been told, assumes that the appropriate
mode of evaluang opons is some form of cost-benet (or cost-eecveness) calculaon across individuals. Public health,
according to this view, appears to permit, or even to require, that the most fundamental interests of individuals be sacriced
in order to produce the best overall outcome. But that oversimplicaon misperceives, that the eld of public health is inter-
ested in securing the greatest benets for the most.
The evoluon of PHE frameworks signies turning to the collecve values and more specied norms such as ulity, evidence
based eecveness, distribuve jusce and fairness, solidarity and social responsibility, community empowerment and par-
cipaon, transparency, accountability and trust that some of them can be considered as mid-level principles. In addion to
distribuve jusce, what should be considered in developing a PHE framework is considering the achievement of well-being
dimensions adequately signies developing healthy social structures, promong individual capabilies, developing ability to
reasoning and strengthening autonomy based on the theory of social jusce.
Public health and ethics are undeniably bound together. Many people in public health even see the muldisciplinary public
health as a moral endeavour: to protect the health of whole populaons and to draw special aenon to the weaker mem-
bers of sociees.
The naonal policy agenda of any naon in front of a pandemic is set and resolved by the compeve interplay of special-
interest groups, but what claims are privileged, which priories are dened and which members of the society are going to
be given the strongest protecon, is an ethical decision made by the policy makers and adhered to (or not) by the general
Humanitarian News
W A B I P N E W S L E T T E R P A G E 14
society.
Ethics in public health cannot turned into concrete measures without taking into consideraon the values of the general so-
ciety as well as that of the parcular communies where the public ethical course of acon is needed. As Kotalik argues
"every discourse about health care has not only a scienc but also a moral dimension, [pandemic inuenza] plans also pre-
suppose certain ethical values, principles, norms, interests and preferences".
Beyond dierent moral theories and a not completely ethical framework developed for public health, the guiding principle
should be the common agreement about the supreme value of a human life. The quest for dignity is universally accepted
and should be a starng point as a guarantee of the respect of human rights. Human rights are shared values. Human rights
are our common possession. When abuses are commied against anyone in any society, the dignity of humanity as a whole
is compromised. When we abandon eorts to sustain human dignity, we forfeit the essenal meaning of being human, and
when we hesitate in our commitment to the idea of human rights, we abandon our moral principles.
On those basis, whichever the policies adopted in order to control a pandemic, the responsible policy-makers should be able
to raonally demonstrate that preserving human life, any and every human life and prevenng premature deaths are their
governing principles. Otherwise, the acceptance that in some circumstance human life is worthy sacricing, would radically
change many of the universal ethical assumpons we uphold today from euthanasia to end of life dilemmas, from resource
allocaon policies to the provision of expensive treatments. Polical leaders must give robust ethically grounded reasons for
any measure that cannot be indisputably grounded in the values enshrined in the Universal Declaraon of Human Rights and
above all, the universal precepts that everyone's right to life shall be protected by law and that human dignity is inviolable
and must be respected and protected in any circumstance. Just because humanity, which is present in even the lowliest of
men, gives each individual a dignity that must be respected by all other individuals, society, and the state. A dignity that can-
not be taken away from us ever, not by anyone.
References:
1. Callahan D et al. Am. J. Public Health. 2002;92(2):169–176
2. Jennings B. Acta Bioethica. 2003; 9:165–176.
3. Kass NE. Am J Public Health. 2001; 91:1776–1782.
4. Kotalik J. Bioethics. 2005; 19:422–431.
5. MacIntyre A. Dependent Raonal Animals: Why Human Beings Need the Virtues. Open Court Publishing, 1999.
6. Mann JM et al. Health Hum Rights. 1994;1(1):6–23
7. Michael L. New Bioethics 20(1):12-34
8. Singer PA et al. Br. Med. J. 2003;327(7427):1342–1344
*The views expressed in this arcle are those of the author (Silvia Quadrelli) and do not necessarily reect the ocial posi-
ons of the Execuve Board or Internaonal Board of Regents of the WABIP.
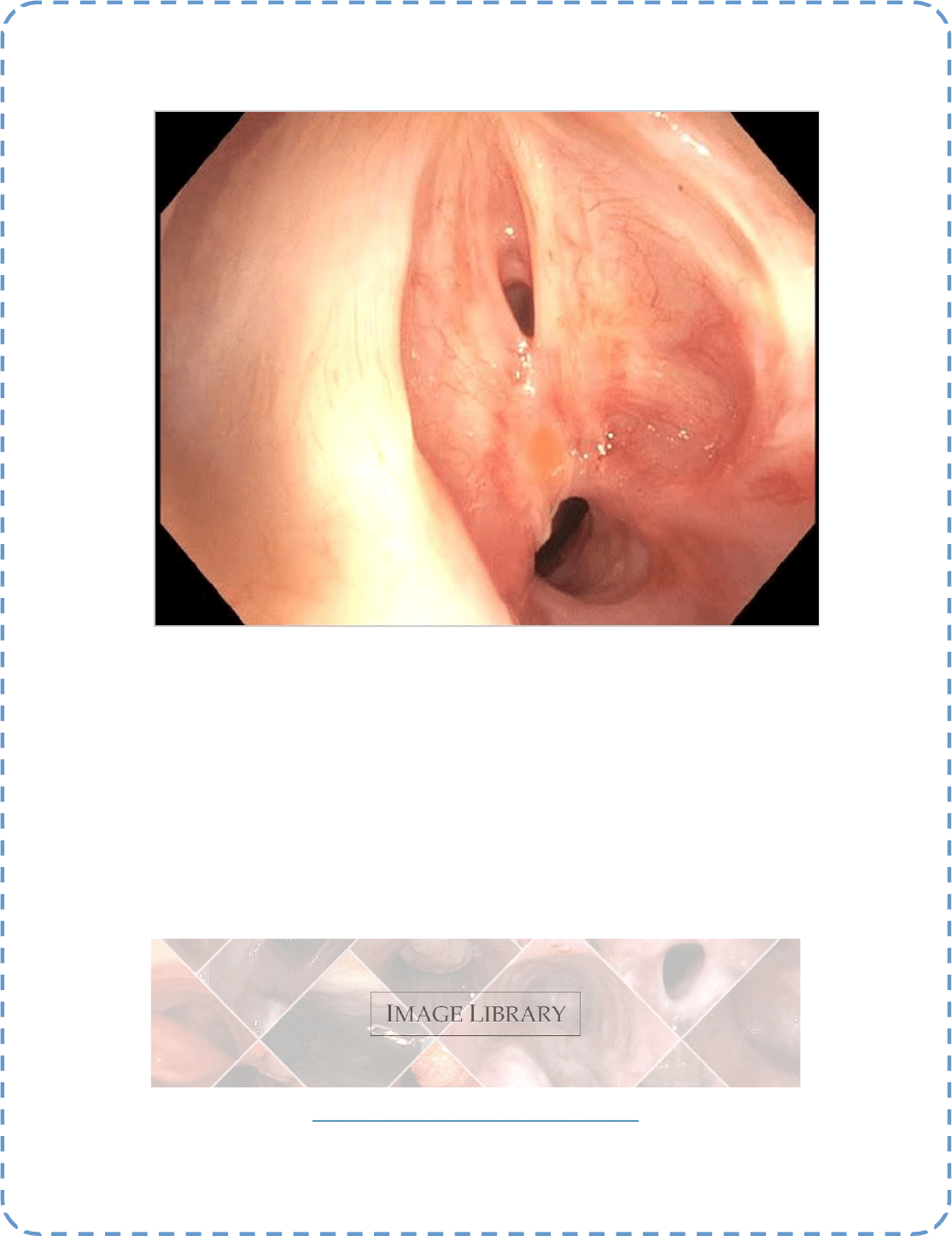
Best Image Contest 2020 Recipient (2 of 3)
Descripon: Proximal airway of a 59 year-old female presenng with 3 months of progressive dyspnea fol-
lowing a non-tramauc intubaon in the seng of surgical resecon of the colon. In this picture, we are visu-
alizing proximal subgloc stenosis that is actually tacking open the true vocal cords (also visualized).
Submier: Dr. Daniel G. Dunlap
*****
This image is 1 of 3 selected among 100+ submissions to our Best Image Contest held in 2019. Please stay tuned to the next Image
Contest, opening later this year!
Find the above image and more at the WABIP Academy Image Library !
hps://www.wabipacademy.com/imagelibrary
Best Image Contest
P A G E 15
Biennial Board of Regents Meeng —We are pleased to announce that the Board of Regents meeng will be held this
September in which BOR members will be able to connect via Zoom teleconferencing. The Vice-chair elecons shall
also take place during this teleconference using anonymous online ballots.
WCBIP 2026 bids & presentaons—The WABIP has postponed 2026 presentaons & vong to WCBIP 2022. In the
coming months, we will re-open and accept addional applicaons for 2026 bids. The Board of Regents shall vote on
the 2026 host site and congress president in April 2022 in Marseille, France.
New member society - We are pleased to announce that the Vietnam Respiratory Society
(VNRS) has joined the WABIP. Please join us in welcoming one of the fastest growing res-
piratory sociees in Southeast Asia. VNRS was established in 2014 as a non-prot organiza-
on dedicated to respiratory work, community and research in Vietnam. We will be part-
nering with VNRS execuve members Prof.Dr. Ngo Quy Chau & Prof. Giap Vu Van in organ-
izing a bronchoscopy workshop co-sponsored by the WABIP at the VNRS annual congress
this November 2020. Society website: hp://hoihohapvietnam.org/en
11th Bronchoscopy Workshop - SCOPE 2020: Intervenonal Pulmonology in Lung Cancer (Philippines)
When: August, 2020
Where: Novotel, Manila, Philippines
Program Director: Ronald A. Fajardo, MD
Program Type: Educaonal seminar (postgraduate may include physicians in pracce and trainees), Hands-on work-
shop, Conference (didacc lectures)
21st World Congress for Bronchology and Intervenonal Pulmonology (WCBIP)
When: September 24-27, 2020
Where: Shanghai, China
President: Guangfa Wang, MD, PhD
Website: hps://www.WCBIP.org
6th European Congress for Bronchology and Intervenonal Pulmonology
When: April 22-24, 2021
Where: Megaron Athens Internaonal Conference Centre - Athens, Greece
President: Prof. Grigoris Stratakos
Website: hp://www.ecbip2021.org/
WABIP NEWS
P A G E 16
UPCOMING EVENTS

Cryobiopsy: Is it worth the risk?
Specimens from transbronchial lung biopsies are usually very small and lack architectural integrity due to crush arfact to diagnose diuse lung
diseases with condence. Transbronchial Lung Cryobiopsy (TBLC) is a novel, minimally invasive technique for obtaining lung ssue for histo-
pathological assessment in Intersal Lung Disease (ILD). The major advantage of this procedure is that larger ssue samples with a higher per-
centage of alveolar ssue can be obtained with fewer crush arfacts and less atelectasis.
The cryosurgical equipment operates by the Joule–Thompson eect, which dictates that a compressed gas released at high ow rapidly expands
and creates a very low temperature. The cooling agent (carbon dioxide or nitrous oxide) is applied under high pressure through the central ca-
nal of the probe. The gas at the p suddenly expands due to the dierence in pressure (relave to atmospheric pressure), causing a drop in
temperature at the p of the probe (in the ssue of approximately −50°C to −60°C). The probe is cooled for approximately 3 to 6 seconds (larger
probe cooled for 7–8 seconds). The frozen ssue aached to the probe’s p is removed by pulling the cryoprobe together with the broncho-
scope. The frozen specimen is then thawed in physiological saline and xed in formalin.
Recently several studies have been published on the feasibility and safety of this technique. The fundamental queson regarding this technique
remains the balance between the risk of complicaons and the benet of geng a beer sample with a higher yield for diagnosis.
A prospecve, mulcenter, diagnosc accuracy study (COLDICE) (1) invesgated diagnosc concordance between TBLC and Surgical Lung Biopsy
(SLB)- the gold standard, across nine Australian hospitals. A muldisciplinary team of physicians decided if the paent needed a lung biopsy to
establish a denive diagnosis. The paents were then referred for a sequenal TBLC and SLB under one procedural setup. Pathologists were
blinded as to the nature of the procedure performed to obtain the samples. A muldisciplinary team of physicians and radiologists then evalu-
ated the pathological report in a blinded fashion with the clinical and radiographic informaon to render the nal diagnosis. Co-primary end-
points were the agreement of histopathological features in TBLC and SLB for paerns of denite or probable usual intersal pneumonia (UIP),
indeterminate for UIP, and alternave diagnosis; and for the agreement of consensus clinical diagnosis using TBLC and SLB at Mul-Disciplinary
Discussion (MDD).
Sixty-ve paents (31 [48%] men, 34 [52%] women; TBLC (7·1 mm, SD 1·9) and SLB (46·5 mm, 14·9) underwent lung biopsies. Samples were
taken from two separate ipsilateral lobes. Histopathological agreement between TBLC and SLB was 70·8%, and the diagnosc agreement at
MDD was 76·9%. For TBLC with high or denite diagnosc condence at MDD (39 [60%] of 65 cases), 37 (95%) were concordant with SLB diag-
noses. In the 26 (40%) of 65 cases with low-condence or unclassiable TBLC diagnoses, SLB reclassied six (23%) to alternave high-condence
or denite MDD diagnoses. Mild-moderate airway bleeding occurred in 14 (22%) paents due to TBLC. The 90-day mortality was 2% (one of 65
paents), following acute exacerbaon of idiopathic pulmonary brosis.
Editor-in-Chief: Dr. Kazuhiro Yasufuku
Research
Primary Business Address:
Kazuhiro Yasufuku, Editor-in-Chief
WABIP Newsleer
c/o Judy McConnell
200 Elizabeth St, 9N-957
Toronto, ON M5G 2C4 Canada
E-mail: newsleer@wabip.com
P A G E 17
Associate editor:
Dr. Ali Musani
Associate editor:
Dr. Sepmiu Murgu
A large metanalysis published in 2017 (2) compared the TLBC with Video-Assisted Thoracoscopic Surgery (VATS) which revealed
that TBLC pooled diagnosc yield was 83.7% (76.9-88.8%), pooled sensivity was 87% (85-89%), and a pooled specicity was 57%
(40-73%). In contrast, VATS pooled diagnosc yield was 92.7% (87.6-95.8%), pooled sensivity was 91.0% (89-92%), and pooled
specicity was 58% (31-81%). The incidence of moderate to severe endobronchial bleeding aer TBLC and of post-procedural
pneumothorax was 4.9% (2.2-10.7%) and 9.5% (5.9-14.9%), respecvely. This metanalysis shows that the diagnosc yield of TBLC is
signicantly lower than the VATS. However, the risk of potenal procedural complicaons, such as pneumothorax and moderate to
severe bleeding, need to be weighed in when considering this procedure.
Another study (3) looking at the complicaons of TBLC demonstrated that out of 257 TBLCs analyzed, complicaons were observed
in 15.2% of paents, and only 5.4% of all paents required hospital admission on the day of the procedure. Hemorrhage was the
most frequent complicaon. In the 30 and 90 days following the TBLC, rates of readmission were 1.3% and 3.5%. No outpaents
died in the rst 30 days. The 30- and 90-day mortality rates were 0.37% and 0.78%, respecvely, but none of the deaths were
linked to the TBLC procedure.
In view of evolving experience and data, TBLC should be considered a specialized procedure that should be oered in centers with
experse and resources to perform the procedure safely. I refer readers to the following recommendaons from the American
College of Chest Physician’s Guidelines, 2020 (4).
• at least two dierent sites (either dierent segments in the same lobe or dierent lobes should be biopsied to ensure ample
ssue acquision
• the biopsy should be performed with the p of the cryoprobe located 1 cm from the pleura
• uoroscopy should be used
• a bronchial blocker either through an endotracheal tube or rigid bronchoscope should be ulized
• a small cryoprobe (1.9 mm) rather than a larger cryoprobe (2.4 mm) should be used
References:
1. Troy LK et al. Lancet Respir Med. 2020;8(2):171-181.
2. Iikhar IH et al. Ann Am Thorac Soc. 2017;14(7):1197-1211.
3. Aburto M et al. Respir Med. 2020 Apr - May;165:105934. doi: 10.1016/j.rmed.2020.105934. Epub 2020 Mar 19.
4. Maldonaldo F et al. CHEST 2020; 157(4):1030-1042
P A G E 18
P A G E
19
WABIP ACADEMY- WEBCASTS
The WABIP has started a new educaon project recently: THE WABIP ACADEMY. The WABIP Academy will pro-
vide free online webcasts with new and hot topics that will interest pulmonologists and intervenonalists.
Current webcast topic: Tissue acquision for biomarker directed therapy of NSCLC
You can reach these webcasts by using this link: hp://www.wabipacademy.com/webcast/
www.bronchology.com Home of the Journal of Bronchology
www.bronchoscopy.org Internaonal educaonal website for
bronchoscopy training with u-tube and
facebook interfaces, numerous teachiing
videos, and step by step tesng and assess
ment tools
www.aabronchology.org American Associaon for Bronchology and I
ntervenonal Pulmonology (AABIP)
www.eabip.org European Associaon for Bronchology and
Intervenonal Pulmonology
W A B I P N E W S L E T T E R
Links
www.chestnet.org Intervenonal Chest/Diagnosc Procedures (IC/DP)
NetWork
www.thoracic.org American Thoracic Society
www.ctsnet.org The leading online resource of educaonal and
scienc research informaon for cardiothoracic
surgeons.
www.jrs.or.jp The Japanese Respirology Society
sites.google.com/site/asendoscopiarespiratoria/
Asociación Sudamericana de Endoscopía Respiratoria
P A G E 19