Volume 06
Issue 01
January 2018
Inside This Issue
Opinion/Editorial, 2
Technology Corner, 3,4
Tips from the Experts, 5,6,7,8,9
Humanitarian News, 10,11
Educaon and Training, 12
BOR News, 13
Research, 14
WABIP Academy Webcasts, 15
Links, 15
Upcoming Events, 16
in thoracic surgery, emergencies in inter-
venonal pulmonology). For each IP
procedure we have included: prior expe-
rience requirements, knowledge, core
basic skills, a check list for procedural
steps for praccal training, resources for
hands-on praccal training and tools for
quantave, qualitave and outcomes
assessment. The whole document is
published in full on the European Associ-
aon for Bronchology and Intervenonal
Pulmonology (EABIP) website. It should
be considered a starng point that will
evolve over me. These standards need
to be reviewed and approved by naon-
al and Internaonal Scienc Sociees
and Healthcare Instuons: the goal is
to improve, disseminate and incorporate
them in healthcare programs. In conclu-
sion, there is a great need for a road
map leading to European standardiza-
on in IP, hopefully a task group funded
by the ERS/EABIP to come up with a
soluon applicable across Europe, so as
to develop an ocial cercaon recog-
nized in the EC (and in post-Brexit UK),
as we have for Specialty Fellowships.
5
References
1. Lamb CR et al. Chest. 2010; 137: 195-
9
2. Mullon JJ et al. Chest. 2017; 151(5):
1114-21
3. Loddenkemper R et al. Breathe.
2006; 3: 59–70
4. Farr A et al. Breathe. 2016; 12(3):217-
20
5. Corbea L et al. Report of the Con-
sensus Conference on Training and
Competence Standards for the Inter-
venonal Pulmonology Master Program
in Italy: www.eabip.org/training
Division of Intervenonal Pulmonology,
Careggi Hospital, University of Florence,
Director of the Training Program and Master
in Intervenonal Pulmonology, Florence
Intervenonal Pulmonology (IP) is experi-
encing a rapid evoluon of new technol-
ogies. Several internaonal projects are
developing standardized training pro-
grams, capable of establishing an Ultra-
Specialty discipline (beyond pulmonary
and crical care fellowships, to be orga-
nized jointly with volume expert centres)
with validated metrics for trainee compe-
tency assessment.
1
A gradual progression
from theory to pracce is envisaged,
using new teaching techniques, including
live sessions, low and high delity simula-
on, non-technical skill training, ipped
classroom models and problem-based
learning (PBL) exercises – to ensure that
trainees’ skills are enhanced and updat-
ed. Europe has a long tradion in IP, with
e.g. Dumon and Cavaliere in rigid bron-
choscopy, Jacobaeus and Boun for tho-
racoscopy, Becker in EBUS: their schools
are sll the centers of excellence for
training in Europe. While the United
States has developed adequate training
standards and oers over 30 IP Fellow-
ships,
2
in Europe training program stand-
ardizaon is patchy. The European Res-
piratory Society (ERS) organizes since
2006 an annual board cercaon in
Pneumology, the “Hermes project”, to
standardize training within dierent dis-
ciplines of respiratory medicine, but not
yet for IP
3
. The ERS does however organ-
ize many advanced training courses in IP
in France, Greece, Italy, Germany and
Denmark and, since 2016, a professional
cercaon of competence in EBUS held
mostly in Heidelberg, Amsterdam and
Copenhagen.
4
The ERS working group on
IP plans to extend this experience to oth-
er skills and procedures, such as thoraco-
scopy and Advanced Thoracic UltraSound
(TUS). Furthermore, individual European
countries hold advanced weekly courses
or “Boot Camps on IP” and structured
Master, e.g. 1 year (500 hours) in Italy, 2
years (130 hrs) in France or in Spain. If a
trainee is interested in IP in Germany, s/
he receives IP training in the endoscopy
unit for 1 year in the best centers (e.g.
Heidelberg, Essen, Hemer or Gaung),
using a simulator for the rst few weeks
and close supervised hands-on training. In
the UK, trainees keep a logbook for 5
years, to be reviewed and signed o peri-
odically by their supervisors; in the Man-
chester region, an online based
“Pulmonary passport” has been intro-
duced, which includes all procedures
(EBUS, Thoracoscopy, etc.). But at present
we do not have a single, common curricu-
lum throughout Europe, nor is a cer-
cate of competence in IP mandatory in
Europe, while a diploma is oen required
when applying for a post. In Italy over the
years we have felt the need to standard-
ize our training program, for the 1-year
Master and also in lifelong training pro-
grams, so that trainees can gradually
achieve full competence in the majority
of IP skills. The teaching faculty on our
Masters worked on a dra standardized
training program, involving the parci-
pang centers: this can guide physicians
who want to improve their own and assist
those organizing IP training programs.
The document includes a general part on
Core Curriculum contents, innovave
training methods and technical and non-
technical simulaon, and a Syllabus de-
scribing the basic issues and skills for each
knowledge base and procedure of IP
(exible bronchoscopy and basic sampling
techniques, intervenonal endosonogra-
phy (EBUS, EUS, EUS-B), bronchoscopic
navigaon and EBUS-radial probe, trans-
bronchial cryobiopsy, transthoracic pul-
monary biopsy, rigid bronchoscopy and
related procedures, sedaon in interven-
onal pulmonology, pleural procedures,
paediatric bronchoscopy, bronchoscopy
in anaesthesiology and ICU, bronchoscopy
Guest Opinion/Editorial
WABIP Newsletter
J A N U A R Y 2 0 1 8 V O L U M E 6 , I S S U E 1
EXECUTIVE BOARD
Zsolt Papai MD
Székesfehérvár, Hun-
gary
Chair
Silvia Quadrelli MD
Buenos Aires, Argen-
na
Vice-chair
Hideo Saka MD
Nagoya, Japan
Secretary General
Hojoong Kim MD
Seoul, Korea
Treasurer
Eric Edell MD
Rochester MN, USA
President WCBIP 2018
Quangfa Wang MD
Beijing, China
President WCBIP 2020
Henri Colt MD
Laguna Beach, CA
Immediate Past-chair
STAFF
Michael Mendoza
General Manager
Judy McConnell
Administrator
Kazuhiro Yasufuku
Newsleer Editor-in-
chief
P A G E 2
European standardizaon prospecve for training
Lorenzo Corbea
Technology Corner
Robocs in Thoracic Surgery: Myths and Realies
Waël C. Hanna, MDCM, MBA, FRCSC,
Division of Thoracic Surgery, McMaster University,
Hamilton, ON, Canada
Introducon: Roboc Thoracic Surgery (RTS) has emerged as the most advanced plaorm for minimally invasive access to the
chest. RTS oers mulple advantages over tradional Video Assisted Thoracoscopic Surgery (VATS), including three-dimensional
visualizaon, increased degrees of freedom of moon, beer ergonomics, and enhanced precision
1
. Over the past decade, the pro-
poron of lung resecons that are being performed by RTS has risen steadily and now comprises close to 10% of all operaons
performed in the United States
2,3
. Although RTS is being rapidly adopted, there remains signicant equipoise about its clinical value
and associated costs. In this arcle, we address 3 myths and realies around RTS compared to VATS.
Background: The rst myth is that RTS lung resecon is associated with beer clinical outcomes when compared to VATS. The
second is that RTS Lobectomy is a beer lung cancer operaon than VATS Lobectomy because it allows for beer lymph node dis-
secon and nodal upstaging. The third is that, considering the high capital and disposable expenses for the roboc plaorm, RTS is
more expensive than VATS.
Clinical Applicaon: Mulple studies, including large database analyses and retrospecve comparave series, have failed to
show any advantages in clinical outcomes such as blood loss, length of hospital stay, or postoperave morbidity and mortality
when RTS is compared to VATS
4-7
. A recent systemac review of the literature conrmed those ndings and has demonstrated
that there are no signicant dierences in the rates of conversion to thoracotomy, prolonged air leak, blood loss, or postoperave
pain between RTS and VATS
3
. There is likely no dierence in short term postoperave outcomes between RTS and VATS. The ergo-
nomic advantages of the roboc plaorm have driven the noon that a beer lymph node dissecon, and subsequently improved
nodal upstaging, can be achieved with RTS lobectomy. This noon has been challenged in the general lung cancer populaon by
the ACOSOG Z0030 trial which demonstrated similar survival between lymph node dissecon and lymph node sampling at the me
of lobectomy
8
. Specically concerning RTS lobectomy, it was demonstrated in a recent retrospecve cohort study that the rates of
nodal upstaging are not beer than what is observed in VATS lobectomy
9
. Although this study was not specically powered for
survival, the results suggest that there is no signicant survival dierence between the two techniques. There is likely no dierence
in the rates of nodal upstaging between RTS and VATS. The roboc plaorm is associated with high upfront capital costs (between
$2-3 million) and ongoing maintenance costs ($150,000 to $250,000 per year). A recent matched analysis of the PREMIER database
comparing RTS to VATS lobectomy showed a higher cost to RTS operaons without any added benet in terms of short term out-
comes
5
. However, a repeat analysis of the same database, published recently by dierent authors, was able to measure a signi-
cant decrease in length of stay, complicaons, and conversions to thoracotomy, thereby jusfying the added cost of the roboc
plarom
10
(this paper was not included in the systemac review discussed above). Another study by a high volume roboc centre
has actually reported a cost advantage to using the roboc plaorm, with a measured accounng prot of $4,750 per paent
11
. It
is important to note that all studies which compare the cost of RTS to VATS do so in a retrospecve fashion and calculate only dol-
lar costs. This type of analysis is by denion incomplete and does not account for ulity, quality of life, and opportunity cost. To
date, there has been no cost-ulity analysis (which is the accepted gold standard in determining cost-eecveness) comparing RTS
to VATS in a prospecve fashion. A prospecve blinded randomized controlled trial comparing RTS to VATS is underway, and
scheduled to complete accrual in 2020. The primary outcome of this trial is cost-ulity, and it will provide useful informaon to
healthcare payors about the feasibility and sustainability of RTS in the long-term. It is unknown whether RTS is more expensive
than VATS, and unl prospecve cost-ulity trials are published, this will remain a point of contenon.
W A B I P N E W S L E T T E R
P A G E 3
Conclusion: Roboc Thoracic Surgery is an advanced plaorm for minimally invasive resecons that will undoubtedly usher a new era of
innovaon in thoracic surgery. Further research is required to determine its role and cost-eecveness.
References
1. Lee BE et al. J Thorac Cardiovasc Surg. 2014;147(2):724-29.
2. Rajaram R et al. Ann Thorac Surg. 2016;101(2):533-40.
3. Agzarian J et al. YSTCS. 2016;28(1):182-92.
4. Park BJ et al. J Thorac Cardiovasc Surg. 2012;143(2):383-89.
5. Swanson SJ et al. J Thorac Cardiovasc Surg. 2014;147(3):929-37.
6. Kent M et al. Ann Thorac Surg. 2014;97(1):236-42.
7. Kwon ST et al. J Thorac Cardiovasc Surg. 2017;154(2):652–59.
8. Darling GE et al. J Thorac Cardiovasc Surg. 2011;141(3):662-70.
9. Lee BE et al. Ann Thorac Surg. 2015;100(1):229-33
10. Oh DS et al. Ann Thorac Surg. 2017;104(5):1733-40.
11. Nasir BS et al. Ann Thorac Surg. 2014;98(1):203-09.
W A B I P N E W S L E T T E R P A G E 4
Tips from the Experts
P A G E 5 V O L U M E 6 , I S S U E 1
Introducon
Lung transplantaon presents a unique challenge when compared to other transplanted organs for a variety of reasons. Dual blood supply
with a lack of a vascular re-anastomosis, a contaminated site, medicaon, physical factors, as well as surgical techniques all play a role in
development of airway complicaons (AC). Airway necrosis, dehiscence, stenosis, malacia and infecons collecvely make up the spectrum
of airway complicaons and have been a signicant and persistent source of morbidity and mortality since the original lung transplant. The
reported rate of anastomoc complicaons ranges from 1.6% to 33%, although most agree with an incidence of approximately 15%-18%.
1
Many potenal reasons exist for this wide range; the lack of a standardized grading system may contribute signicantly. Approximately 35%
of paents with a previously treated airway complicaon will experience a second, and the chance of three or more aer the second is ap-
proximately 70%.
2
Frequent oce visits, the need for procedures, hospitalizaons, and addional medicaons can be a nancial and me
burden and minimize the perceived benet of transplant.
The recognion and management of airway complicaons varies based on the me from transplant, locaon of the lesion, and severity.
Instuon specic protocols also account for variance in surveillance, diagnosis, and management. Complicaons can be classied tempo-
rally (early or late), by cause (ischemia, infecon, iatrogenic, or idiopathic), anatomically (anastomoc or post-anastomoc), or descripvely
(necrosis, dehiscence, stula, infecon, stenosis, granulaon ssue or malacia). This arcle reviews a brief history of transplant airway com-
plicaons, transplant-specic anatomy and surgical technique, risk factors for AC, classicaon of AC and management strategies for the
various types of complicaons.
Risk Factors
The eology of AC is undoubtedly mul-factorial. Surgical factors and ischemia of the donor bronchus was inially felt to be primary driver,
however more complex interplay between donor and recipient characteriscs, surgical technique, post-operave recovery, infecons, and
medicaon selecon play a role.
Risk factors for the development of AC have been idened; including procurement aer extended donor mechanical venlaon (50-70
hours) as well as taller recipients.
3
Taller recipients are likely related to surgical technique, as the airway is telescoped with intussuscepon
leading to entrapment of organisms and an increased ischemia risk.
Indicaons and Planning:
Necrosis and Dehiscence
Post-transplant airway necrosis related to ischemic injury is common. The mucosal slough can extend from the anastomosis to lobar or seg-
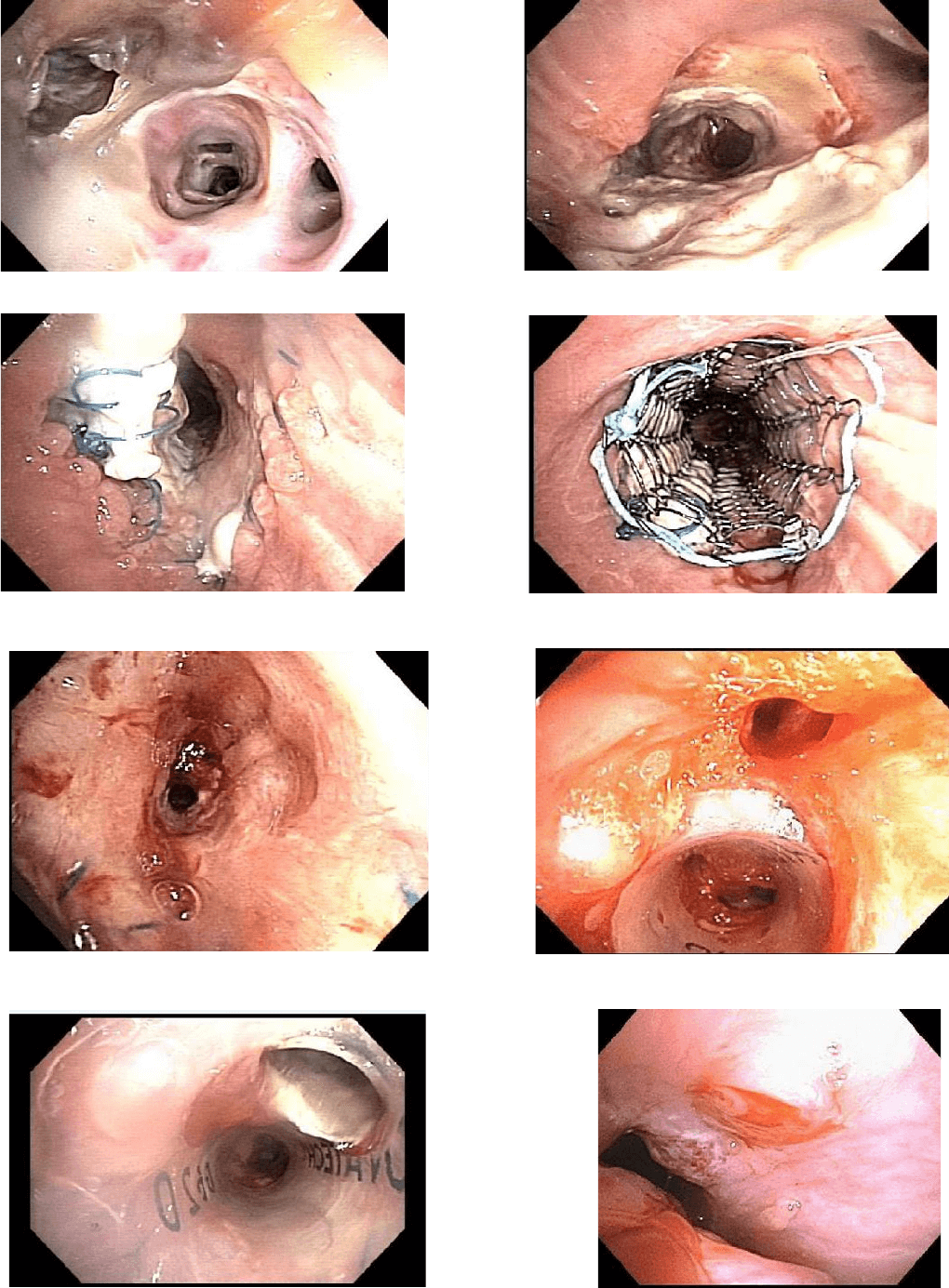
mental levels (Figure 1, 2). Necrosis typically resolves by the sixth week post-transplant and dehiscence occurs when normal healing fails
(Figure 3). Necrosis and dehiscence represent a connuum from healing to catastrophic airway complicaons.
True dehiscence is uncom-
mon but rates are reported from 1- 24%, the lack of standardizaon complicates this.
4
Bronchial dehiscence is oen seen at surveillance bronchoscopy but must be considered with a prolonged air leak, spontaneous pneumo-
thorax, failure to wean, or sepsis. Chest radiographs are unreliable. Computed tomography may be helpful showing bronchial wall defects,
airway debris, or extra luminal air consistent with dehiscence but bronchoscopy remains the gold standard.
A full review of medicaons is too detailed for this brief piece but Sirolimus merits discussion. It is a potent immunosuppressive and anpro-
liferave with less renal impairment, appealing for lung transplantaon. Catastrophic airway complicaons occurred when used in the early
postoperave period. Two separate studies of sirolimus in de novo lung transplant paents describe severe wound-healing complicaons
Airway Complicaons Aer Lung Transplantaon
Michael Machuzak, MD
Department of Pulmonary, Allergy, and Crical Care
Respiratory Instute
Cleveland Clinic
Laura Frye, MD
Department of Pulmonary and Crical Care
Transplant Instute
University of Chicago
P A G E 6 V O L U M E 6 , I S S U E 1
with dehiscence, one resulng in a fatal event. Present recommendaons are to delay using Sirolimus unl complete bronchial wound heal-
ing, typically 90 days aer transplantaon.
5,6
Mucosal slough without necrosis of the bronchial wall may respond to a conservave approach or surveillance and as needed debulk-
ing. Oen anbioc or an-fungal regimens, including inhaled therapies, are iniated. When healing fails and dehiscence occurs, either a
surgical or bronchoscopic intervenon is required. Both have associated morbidity and mortality. Surgical opons include reanastomosis,
ap bronchoplasty, and rarely retransplantaon.
Bronchoscopic techniques include cyanoacrylate glue, growth factors, and autologous
platelet-derived growth factors; however the overall success is poor.
7
A novel technique of placing an uncovered self-expanding metal stent (SEMS) temporarily to facilitate healing exists. This technique ulizes
the tendency for SEMS to iniate granulaon ssue formaon. The SEMS is deployed across the dehiscence and once granulaon ssue and
epithelializaon occurs a stent exchange (if the defect is sll present) or removal (if healed) is performed, typically within a few weeks (Figure
4). Mean me to stent removal was 37.5 days.
8
Precise placement and removal make this method challenging with the potenal to extend
the injury. Close surveillance is recommended given the tendency for stenosis or malacia to occur at or distal to the site of prior dehiscence.
Fistula
Bronchial stulae are challenging but fortunately rare and can occur as communicaons between the airway, pleura, mediasnum, or vascu-
lature. Fistula may present as dyspnea, sepsis, pneumothorax, subcutaneous emphysema, or a persistent air leak typically in the seng of
dehiscence. Management is similar to that of anastomoc dehiscence. Success depends on the locaon and size of the defect.
Bronchovascular stulas are rare and oen fatal. Erosion from any infecon, parcularly aspergillus, is most typical.
A herald bleed must be
evaluated quickly. Case reports of surgical management with pneumonectomy (if bilateral transplantaon), bilobectomy, or stula resecon
and reconstrucon have been successful.
9
Anastomoc infecons
Infecous complicaons are common, parcularly in the rst 3 months, and will be seen in nearly seventy-ve percent of transplant recipi-
ents with bacterial pneumonia being most common. Immunosuppression, ischemic complicaons, impaired mucociliary clearance, impaired
lymphac drainage, poor cough reex due to denervaon, and the direct communicaon of the allogra with the environment all play a
role.
10
Pre-transplant colonizaon is also common.
Infecons at the anastomosis are a complicaon but more importantly are oen the precursor to issues covered later. Diagnosis usually oc-
curs at bronchoscopy. Inammaon, ulceraon, or pseudomembranes are oen seen along the airway and are treated with debridement
and anbiocs. Protocols vary by instuon and include systemic and inhaled regimens with voriconazole, itraconazole, and inhaled ampho-
tericin commonly used.
Bronchial Stenosis
Bronchial stenosis is the best described complicaon; with reported rates ranging from just over 1% to as high as one third.
1
They can be
anastomoc or distal. (Figure 5). Non-anastomoc stenosis can be technically challenging as they can extend into segments. The bronchus
intermedius is the most commonly involved non-anastomoc site, referred to as vanishing bronchus intermedius syndrome (VBIS).
11
The eology may involve infecon, inammaon, or ischemia and can result in remodeling. Paents present with dyspnea, drop in spirome-
try, cough, wheeze, or recurrent episodes of pneumonia. Chest radiography can be the rst indicator with luminal compromise or atelectasis.
CT of the chest can reveal xed bronchial narrowing. Diagnosis by exible bronchoscopy remains the gold standard.
The management of bronchial stenosis oen requires a stepwise, mulmodality approach. Successful techniques include dilaon, ablaon,
and stent placement. Dilaon can be by balloon or rigid dilaon. Dilaon by balloon is oen the rst therapeuc maneuver performed and
provides excellent results with relief of symptoms and improved spirometry. The stenosis oen recurs aer dilaon, but repeated balloon
dilaons may be the only intervenon required in 26% of cases.
12
While no studies have compared methods, balloon dilaon has several
advantages. It can be performed via exible bronchoscopy and under conscious sedaon. Balloons come in mulple sizes and lengths allow-
ing for specic selecon. Lastly, balloon dilaon allows for a rapid increase in the size of the balloon rather than repeated upsizing of the
rigid bronchoscope. Rigid dilaon has several advantages over balloon bronchoplasty such as expense (oset by the need for general anes-
thesia), direct visualizaon during dilaon and uninterrupted venlaon. Perhaps the largest benet of the rigid bronchoscope is the ease of
stent placement if a silicone stent is to be placed.
13
Tips from the Experts
Tips from the Experts
P A G E 7 V O L U M E 6 , I S S U E 1
In cases where a focal web-like stricture is found, a mucosal sparing technique such as electrocautery or laser should be employed followed
by dilaon. Techniques reported include those previously reported including: cryotherapy, electrocautery, argon plasma coagulaon, laser,
brachytherapy, or photodynamic therapy.
13
Topical applicaons of mitomycin-c or submucosal applicaons of steroids have also been used. There are no controlled trials of these inter-
venons, however literature supports that the use of these therapies may potenally delay the me to re-stenosis.
14
If the stenosis is recurrent, stenng may be required. This is a dicult decision as stent complicaons can be signicant. The technical aspects
of a complicated anastomosis has led some to favor placement of self-expanding metal stents (SEMS) However, while SEMS provide immedi-
ate relief as well as some protracted success they are fraught with long-term complicaons and must be carefully considered.
7,8
The issues with SEMS make silicone stents generally favored for the management of benign stenosis as they have advantages of the ease of
reposioning, removal and reduced granulaon ssue formaon (Figure 6). They are more prone to migraon and require rigid bronchosco-
py for placement and removal but can be customized to length, diameter or “notched” on site (Figure 7). Data suggests no increase in com-
plicaons of customized stents for complex airway diseases.
15
Issues with stent placement and complicaons have led to the development of new technologies, including 3-D printed or biodegradable
stents (BDS). Biodegradable stents are well tolerated and completely dissolve aer months. In one prospecve study of BDS, eleven stents
were placed in ten paents. All had improved spirometry and airway patency was achieved in 9/11 at 1-year follow-up with complete degra-
daon aer 141 days.
16
3-D reconstructed stents may play a role in transplant airway complicaons as they allow for a personalized t.
In paents with recalcitrant stenosis alteraon of immunosuppression with the addion of sirolimus can be considered (once airway healing
has occurred). A retrospecve review of 10 paents with recurrent stenosis reported 8 of 10 paents achieved airway patency within 3
months and 7 of 10 had a signicant response within the rst month of starng rapamycin.
7,8
A muldisciplinary approach is ideal and if endoscopic therapy fails, a surgical approach should be considered. An invasive approach is risky
but somemes required, with bronchial anastomosis reconstrucon, bronchoplasty, sleeve resecon, lobectomy, pneumonectomy, and re-
transplantaon all described.
Excessive Granulaon Tissue
Occluding endoluminal granulaon ssue occurs in up to a quarter of lung transplant recipients, most commonly at the anastomosis. Airway
infecon, parcularly with aspergillus, can exaggerate this.
17
Progressive dyspnea, cough, diculty clearing secreons, post-obstrucve pneu-
monia, or hemoptysis may be the presenng symptoms. Reduced spirometry or a chest CT showing obstrucve granulaon ssue may be
seen but bronchoscopy remains the gold standard.
Forceps can remove granulaon ssue easily, but in some cases the beveled edge of the rigid bronchoscope is required to quickly restore
patency. Heat or cold modalies as well as the micro-debrider can be used to restore patency. A superior safety prole, the cryosensivity
of granulaon ssue, excellent hemostasis and the ability to use around stents without the risk of ignion even in high concentraons of oxy-
gen make cryotherapy an appealing opon. APC, electrocautery, and laser ablaon have a long history of successful management. High
dose rate (HDR) endobronchial brachytherapy, or photodynamic therapy have also been reported but should be used with extreme cauon
as serious complicaons including fatal hemoptysis, have been described.
18
Endobronchial applicaon of anbrocs (Mitomycin) or injecon of an-inammatory agents has been described in the management of
granulaon ssue with limited success. Although randomized trials are lacking, anecdotal success and excellent safety prole encourage con-
nued usage. Bronchial stents have been reported to improve patency in refractory cases but can promote granulaon ssue.
Stent place-
ment is complicated by granulaon in 12 to 36% of paents.
19
Tracheobronchomalacia
Malacia of the airway presents in a myriad of ways. A “barking” cough, diculty clearing secreons, or a drop in spirometry more marked
during expiraon are typical. Signicant malacia is dened as luminal narrowing of 50% or more on expiraon (Figure 8).
20
The management is extrapolated from the non-transplant populaon. Aggressive pulmonary hygiene, mucolycs, and non-invasive posive
pressure venlaon are tried rst. Stenng may improve spirometry if medical management fails. Stenng should be carefully considered.
11
If pursued, silicone stenng is typically preferred by experts with close surveillance and oen a stent-free trial aer 6-12 months.
P A G E 8 V O L U M E 6 , I S S U E 1
Quality Control: Classicaon of Airway Complicaons
A potenal reason for the wide range of reported AC may be the lack of a standardized, well-accepted grading system. Early grading systems
relied on bronchoscopic inspecon with some excellent ndings including predicon of subsequent anastomoc complicaons; however they
were subjecve and captured only early complicaons. This shortcoming was later addressed. Subsequent addions included bronchial stric-
tures, suture status, and presence of granulaon ssue, dehiscence or malacia. The most recently proposed system, by Dutau and colleagues
known as the MDS grading, approaches AC in a slightly dierent manner. Unique to this approach is the ability to include the extent of the
abnormalies, from the suture line to more distal lobar and segmental levels.
The M designaon describes the macroscopic appearance ran-
ging from normal healing to include carlaginous protrusion, granulaon or necrosis. The D classicaon describes airway diameter and the S
designaon assesses the suture line for dehiscence and ranges from the absence to a full dehiscence.
21
A universally accepted classicaon system is the rst step allowing for scienc study and consistent reporng to truly dene the incidence,
prevalence, morbidity and mortality. A taskforce of the Internaonal Society of Heart and Lung Transplant has recently completed such a
classicaon system with results soon to be published.
Bronchial Artery Revascularizaon
Roune lung transplantaon does not reestablish bronchial artery circulaon leaving the anastomoc site dependent on retrograde ow.
Anastomosis of bronchial arteries has been successful with promising short and long term results.
A pilot study at the Cleveland Clinic looked
at a series of 131 lung transplant paents who underwent BAR with an overall success rate of 90% including a 95% success in bilateral trans-
plants. Bronchial artery patency was associated with uniformly normal airway healing. The 5 and 10-year survival for bilateral lung transplant
was superior for BAR paents. A higher risk of bleeding was seen, not aecng safety.
22
While encouraging, mul-center studies are needed
to establish these benets.
Summary
In paents with advanced pulmonary disease, lung transplantaon can improve survival and quality of life. However, airway complicaons
remain a major obstacle with associated morbidity and mortality. Paents with AC need addional visits, procedures and adjustments of
medicaons. The increased need for care in an already complicated regimen can lead to a lower perceived improvement in quality of life.
This can be discouraging, costly, and me-consuming. Recent improvements in donor and recipient selecon, surgical technique, periopera-
ve management, and immunosuppression have decreased the incidence of AC.
The management of lung transplant associated airway complicaons is complex. Many therapeuc opons exist and there is no strong data
to suggest one is superior. Management is best delivered in a muldisciplinary approach performed by individuals experienced in the above
techniques with an understanding of the intricacies of the post-transplant paent.
References
1. Machuzak M et al. Curr Opin Organ Transplant 2010; 15: 582-7
2. Murthy S et al. Ann Thorac Surg 2007;84: 401-9
3.Van De Wauwer C et al. Eur J Cardiothorac Surg 2007; 31: 703-10
4. Garfein ES et al. J Thorac Cardiovasc Surg 2001; 121(1): 149-54
5.Groetzner J et al. J Heart Lung Transplant 2004; 23(5): 632-8
6.King-Biggs MB et al. Transplantaon 2003; 75(9): 1437-43
7. Maloney JD et al. Ann Thorac Surg 2001; 82(6): 2109-11
8.Mughal M et al. Am J Respir Crit Care Med 2005; 172: 768-71
9.Knight J et al. J Heart Lung Transplant 2008; 27: 1179-85
10. Ahuja J et al. Radiol Clin North Am 2014; 52(1): 121-36
11. Santacruz JF et al. Proc Thorac Soc 2009; 6(1): 79-93
12. Chhajed PN et al. Chest 2001; 120(6): 1894-9
13. Machuzak M. In: Principles and pracce of intervenonal pulmonology. New York: Springer Science + Business Media; 2013. p463
14. Cosano-Povedano J et al. J Bronchology Interv Pulmonol 2008; 15(4) 281-3.
15. Breen DP et al. Respiraon 2009; 77(4): 447-53
16. Fuehner T et al. Transplant Internaonal 2013; e58-60
17. Mulligan MS. Chest Surg Clin N Am 2001; 11(4): 907-15
18. Tendulkar RD et al. Int J Radiat Oncol Biol Phys 2008; 70(3): 701-6
19. Saad CP et al. Transplantaon 2003; 75(9): 1532-8
20. Simo M et al. Thoracic endoscopy. Advances in intervenonal pulmonology. Malden (MA): Blackwell Publishing; 2006
21. Dutau H et al. Eur J Cardiothorac Surg 2014; 45: 33-38
22. Peerson, GB et al. Curr Opin Organ Transplant 2010; 15: 572-7
Tips from the Experts
Tips from the Experts
P A G E 9 V O L U M E 6 , I S S U E 1
Figure 1: Necrosis and stenosis of the distal RBI and RML
Figure 2 : Mild necrosis of the right mainstem anastomosis
Figure 3 : Dehiscence of the right anastomosis, note the loose su-
tures and separaon of the donor bronchus
Figure 4 : SEMS placed to iniate granulaon ssue for a dehiscence
Figure 5 : Right Bronchus Intermedius stenosis Figure 6 : Right mainstem stenosis aer dilaon and stent place-
ment
Figure 7: Customized stent placement ; note the
notch for the RUL stent
Figure 8 : Malacia of le mainstem
Humanitarian News
W A B I P N E W S L E T T E R P A G E 10
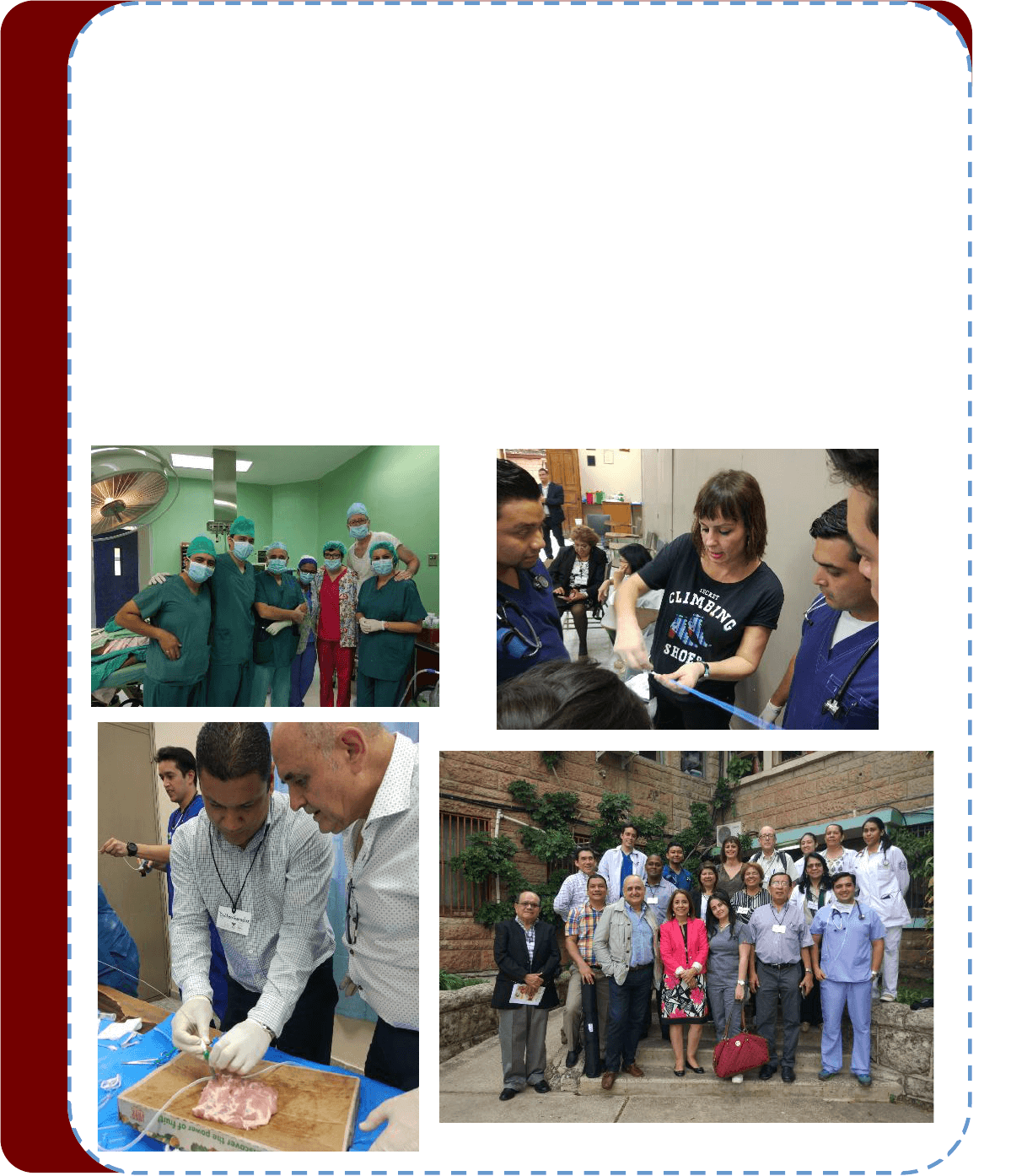
The “Proyecto Horizonte” is an iniave between the World Bronchology Foundaon and SEPAR Solidaria, born in 2015.
Between the 12th and 26th of November, the “Proyecto Horizonte Honduras 2017” resumed its acvity. Dr. Manuel Núñez,
Dr. Enrique Cases, and nurse Merce Cuña, travelled to Tegucigalpa (Honduras) to accomplish 5 objecves, which were 1) to
support the apprenceship of future pulmonologists in Honduras, 2) to make a Second Theorecal and Praccal Cen-
troamerican Course with the engagement of pulmonologist from countries near Honduras, with the aim of updang the
pleural and bronchonscopic techniques, 3) to aend to paents, 4) to donate an an ultrasound machine to the “Instuto
Nacional CardioPulmonar”, and 5) to control the donated material in Nicaragua one year ago.
Specialists from Honduras, Guatemala, San Salvador and Panamá took part in the Second Theorecal and Praccal Course of
Intervenonist Pulmonology. The experience was rewarding and the level of the course, with the involvement of specialist
from Honduras, was very high. The praccal part helped for the apprenceship of the assistants and was highly valued. It is
important to highlight the high level of parcipaon in the nursing sessions -a constant in this Centroamerican Course-,
which shows that nursing raises concerns and arms the necessity of training and smulang it. The work and eorts of
Merce Cuña during the course and in the Instuto asistencial was very outstanding and appreciated.
Humanitarian News
W A B I P N E W S L E T T E R P A G E 11
During our stay in the Instuto, we acvely parcipate in the dierent assistance acvies, complex procedures and forma-
ves and clinic sessions that were organized. The contribuons made were highly valuated. We have to highlight again the
acvity developed by Merce Cuña, above all in encouraging the nursery, and the work of Manuel Cuña in forming future pul-
monologist in Honduras, as well. At the same me, it is important to appreciate the facilies that Dra Suyapa Sosa gave to
us, not only by leng us develop our acvity, but also by bringing us the opportunity of constantly being with pulmonology’s
residents.
In the rst visit to Honduras, because of the high quanty and complexity of pleural pathology in the medical centre, it was
consider that there was a priority need of an ultrasound machine for studying the pleural pathology. Because of this, SIM-
MEDICA donated an echograph with a high-resoluon linear and mini-convex transductcers. We would like to thank the
complete willingness of SIMMEDICA to donate material for the Proyectos Horizonte, it has become a key contributor in these
projects.
Controlling the donated material its fundamental, not only to know that it remains in good condions and that is being cor-
rectly used, but also to let the responsible people of these material feel that World Bronchology Foundaos and Separ Soli-
daria the connues supporng them. Because of that, a visit to Chinandega (Nicaragua) was made, and it was checked that
the donated bronchoscope in September 2016 was being used correctly and that remained in good condions. It is im-
portant that the interns of SEPAR Solidaria in Nicaragua resort to this hospital, where Dr. Amaya, who is the head of the pul-
monology department in the hospital, will receive them cordially.
The use of the allowed material in the Hospital Militar de Managua it is being very useful for the paents. The rst results of
the transbronchial lung cryobiopsies and central airway obstrucon recanalizaon, have been submied. Moreover, the pul-
monologist in charge of the department, Dr. Chrisan Sánchez, stayed for three weeks in Spain –Fundación Jimenez Díaz and
Hospital Universitario y Politécnico La Fe- with a grant from the WBF and Asociación Española de Endoscopia Respiratoria
(AEER), in order to improve its knowledge in intervenonist pulmonology procedures. Dr. Chrisan feels highly inspired, and
is conscious that the development of the intervenonist pulmonology depends to a large extent on him.
This Proyecto Horizonte its possible thanks to many people. Between them, can be named, Dr. Julio Ancochea, who is sensi-
ve and commied with this project, which began in 2015. Thanks to him, SEPAR Solidaria has facilitated the necessary
framework to make the Proyecto Horizonte known in all Centre America. Javier, Luisa, Harold and Gerardo, who are the fu-
ture pulmonology residents in the Instuto Nacional CardioPulmonar, who are enthusiasc for learning, and who are always
sensive and warm with us. Dra. Suyapa Sosa, who is the core of this group. Without her, the Project would have been im-
possible and pointless. Drs. Judy Enamorado, Carlos Alvarado, José Castro, Leslie Padilla, Elías and the nurse Walleska and
other persons who have help and encourage us. To all of them, thank you very much, we always bring back home more
things than what we leave there. Finally, recognizing the generosity, kindness and willingness of SIMMEDICA, without them
it would be really dicult to donate material of good quality, with such an ecient cost.
*The views expressed in this arcle are those of the author and do not necessarily reect the ocial posions of the Execuve
Board or Internaonal Board of Regents of the WABIP. Dr. Enrique Cases is the chair of the World Bronchology Foundaon.
In September 2017, Dr. Henri Colt, with Doctors Maria Simon (Romania) and Mihai Olteanu (Romania), conducted a Train-the-Trainer program
with its aached Introducon to Flexible Bronchoscopy Courses for physicians in the Balkans. Organized and hosted by Dr. Spasoje Popevic
(Belgrade, Serbia) and the University Hospital of Pulmonology, Clinical Center of Serbia in Belgrade, the program included invited leaders from
Serbia, Moldavia, Bulgaria, Macedonia, and Bosnia. These experienced bronchoscopy teachers came together to discuss competency-oriented
pracces, and to enhance their teaching skill using checklists, assessment tools, and case-based 4 box approach exercises in a muldimensional
instruconal program. Role-playing exercises were used to pracce individualized, learner-centric teaching techniques, and several technical
skill staons comprised of airway models were helpful for learning to teach inspecon bronchoscopy using our me-tested step-by-step tech-
niques.
During the Introducon to Flexible Bronchoscopy course (IFB), trainers were able to apply their newfound skills and increased understanding of
the Bronchoscopy Internaonal/WABIP philosophy. They then shared cognive, technical, experienal, and aecve knowledge with more
than 20 IFB course parcipants. Parcipants in the IFB program were, for the most part, junior specialists from local and regional medical cen-
ters, although several surgeons from Serbia were also present, providing helpful insights and clinical experience.
Dr. Spasoje Popevic, now a BI Cered Instructor, provided key leadership during the enre program. In addion to enhancing teaching skills,
trainers discussed educaonal philosophies, and ways to overcome exisng obstacles to implemenng the widespread use of assessment tools
and checklists in the Balkans. An excing “spirit of collaboraon” immediately ensued during the program, and enthusiasc Serbian leaders are
already well into the process of translang The Flexible Essenal Bronchoscopist and several checklists and assessment tools. The Informed
Consent summary page (downloadable from www.bronchoscopy.org) is already translated and being distributed with great success. Mean-
while, leaders from Macedonia, Serbia, Romania, Bulgaria, Moldavia, and Bosnia are moving forward with establishing competency-oriented
training guidelines to complement the apprenceship models currently in place in their respecve pulmonary sociees.
Once more, a direct result of this training program was increased collaboraon and true friendship among colleagues who share a common
interest, colleagues who are able to discard personal egos in order to work together for a greater good, and ulmately, greater benet to their
paents who will may no longer suer from the consequences of procedure-related training. The Bronchoscopy Internaonal team and WABIP
wish to congratulate al these leaders, who, as proacve agents of change, are consolidang the educaonal paradigm shi from a tradional
apprenceship model to a competencyoriented model using assessment tools, checklists, simulaon, and a muldimensional, learner-centric
approach to skill development.
Education and Training
P A G E 12
Figure 1: Leaders from Serbia,
Bosnia, Moldavia, Bulgaria, and
Macedonia discussing denions
of paent suering and roles for
cometency-oriented training at
the Belgrade Train-the-Trainer
seminar
Figure 2: Doctor Marija Zdra-
veska from Macedonia using a
(instructor) hands-o student
(hands-on) approach to teaching
bronchoscopy step-by-step while
working with parcipants in the
Belgrade Introducon to Flexible
Bronchoscopy
Figure 3: Drs. Maria Simon
(Romania), Henri Colt (USA), Spaso-
je Popevic (Serbia), and Mihai Ol-
teanu (Romania) were faculty at
the Trainthe-Trainer program held
in Belgrade, Serbia in September,
2017.
Figure 4: Train-the-Trainer and
Introducon to Flexible Bron-
choscopy Course parcipants
in Belgrade
Bronchoscopy Educaon Project Acvity in Belgrade, Serbia
WABIP NEWS
P A G E 13
2024 WCBIP Host Applications – This is a reminder that applications for hosting the 2024 WCBIP
congress are now open. This is an excellent opportunity for you and your colleagues to host and
organize WABIP's biennial scientific event in your city. Visit the link to read more about the
application process https://www.wabip.com/news/324-call-for-2024-wcbip
Left: Dr. George Eapen (AABIP); Right: Dr. Luis Gonzalo Ugarte Fornell (Ecuador IP Society)
Member Society Spotlight - Since its founding in 1992, the American
Association for Bronchology and Interventional Pulmonology (AABIP) has
been a unifying source for information regarding the fields of Bronchology
and Interventional Pulmonology. Over the last few years, the AABIP has
achieved significant milestones, including having the Journal of Bronchology
and Interventional Pulmonology become indexed on Index Medicus, having
IP Fellowship programs become part of the National Residency Match
Program, running twice-yearly scientific symposium and developing and
implementing the first Board Certification Exam in Interventional Pulmonology. For more information
about this association, please visit: https://aabronchology.org
Reduced registration fees for the 2018 WCBIP/WCBE are still available. Register Today!
Call for Nominations for Next WABIP Vice-Chair
–
Nominations for the next WABIP Vice-chair are still
open. The Vice-chair is a voting member of our Executive Board and is entitled to all rights and
privileges therein. This member shall carry out leadership responsibilities and tasks in accordance
with the principles and objectives of the WABIP to assure the continued growth of our organization.
The current Vice-chair will assume the position of Chair immediately after the current Chair's tenure.
Send us your nominations at https://www.wabip.com/news/323-wabip-vice-chair-2018
New Board of Regents Members
–
We are pleased to welcome Dr. George Eapen (AABIP) and Dr. Luis
Gonzalo Ugarte Fornell (Ecuador IP Society) on the WABIP Board of Regents (“BOR”). With now 57
members, the BOR will meet in Rochester this June to take part in and vote on the next WABIP Vice-
chair, the 2024 WCBIP host site and other important WABIP business.
Biodegradable and Drug Elung Airway Stents
It's like a tailored suit, just for you
Ideal airway stents have been a topic of every major Intervenonal Pulmonology discussion, conference, and a book for over a decade. The de-
nion of an ideal airway stents broadly encompasses, easy to deploy, easy to remove, minimal to non-granulaon forming, and aordable. Bio-
degradable material of stent was included in the wish list as the me went on.
In the last few years, the technology has made possible just about all the above-menoned qualies and much more in the airway stents. Now,
we can order a stent designed according to the measurements, contours, and bifurcaons of a specic airway of a parcular paent. A 3D print-
er can create such a stent in a short period. We can also choose one of many biodegradable materials for the specic longevity of the stent aer
which the stent dissolves and disappears. The pre-specied life of the stent precludes unnecessarily prolonged irritaon of the airway epitheli-
um which leads to brosis and formaon of strictures of the airways. Furthermore, the material used to construct the stent can be impregnated
with chemotherapeuc or an-broc agents which are slowly released locally giving a very high concentraon of the drug locally and drama-
cally low levels systemically thus minimizing systemic toxicity and side eects.
In a European pilot study (1) of biodegradable stents manufactured with bio-absorbable Polydioxanone (PDS), the stents were placed in post-
lung transplant paents with airway strictures. These stents were found to be easy to deploy and due to their biodegradable material, did not
require removal. They served their purpose for a predetermined period with good radial force and tensile strength maintaining patency in the
majority of the airways without any short or long-term complicaons.
In an animal study (2), biodegradable and drug elung stents were implanted in the trachea to study various properes of the stent. The stents
were made of Polycaprolactone and impregnated with Cisplan as the chemotherapeuc agent. The local concentraon of Cisplan was very
high while the systemic levels of the drugs were minimal. The drug slowly released over approximately four weeks and stent disintegrated over
me without any airway strictures.
These customized and individualized stents carry a broad potenal of maintaining patency of the benign and malignant airways while awaing
denive treatments and also providing localized therapy for malignant endobronchial or peribronchial diseases with minimal systemic eects.
It seems like we are very close to having an "ideal stent" if we are not there already.
References
1. Lischke et al. Eur J Cardiothorac Surg. 2011; 40(3):619-24
2. Chao et al. Chest 2013; 144(1):193-9
Editorial Staff
Associate editor: Dr. Ali Musani
Associate editor: Dr. Sepmiu Murgu
Editor-in-Chief: Dr. Kazuhiro Yasufuku
Research
Primary Business Address:
Kazuhiro Yasufuku, Editor-in-Chief
WABIP Newsleer
c/o Judy McConnell
101 College St., TMDT 2-405
Toronto, Ontario M5G 1L7
Phone: 416-581-7486
E-mail: newsleer@wabip.com
P A G E 14
P A G E
15
WABIP ACADEMY- WEBCASTS
The WABIP has started a new educaon project recently: THE WABIP ACADEMY. The WABIP Academy will pro-
vide free online webcasts with new and hot topics that will interest pulmonologists and intervenonalists.
Current webcast topic: Tissue acquision for biomarker directed therapy of NSCLC
You can reach these webcasts by using this link: hp://www.wabipacademy.com/webcast/
www.bronchology.com Home of the Journal of Bronchology
www.bronchoscopy.org Internaonal educaonal website for
bronchoscopy training with u-tube and
facebook interfaces, numerous teachiing
videos, and step by step tesng and assess
ment tools
www.aabronchology.org American Associaon for Bronchology and I
ntervenonal Pulmonology (AABIP)
www.eabip.org European Associaon for Bronchology and
Intervenonal Pulmonology
W A B I P N E W S L E T T E R
Links
www.chestnet.org Intervenonal Chest/Diagnosc Procedures (IC/DP)
NetWork
www.thoracic.org American Thoracic Society
www.ctsnet.org The leading online resource of educaonal and
scienc research informaon for cardiothoracic
surgeons.
www.jrs.or.jp The Japanese Respirology Society
sites.google.com/site/asendoscopiarespiratoria/
Asociación Sudamericana de Endoscopía Respiratoria
P A G E 15
P A G E
16
W A B I P N E W S L E T T E R
P A G E 16
Upcoming Events
IP National Update 2018
When: February 24-25, 2018
Where: Hotel Radisson Blu, Nagpur, India
Program Director: Dr. Sameer Arbat, MD
Program Type: Educational seminar (postgraduate may include physicians in practice and trainees),
Hands-on workshop, Conference (didactic lectures)
Website: http://www.ipnationalupdate2018.com
Faculty Development Program & Introduction to Flexible Bronchoscopy
When: March 1-3, 2018
Where: Auckland, New Zealand
Program Director: Henri Colt, MD
Program Type: Educational seminar (postgraduate may include physicians in practice and trainees),
Hands-on workshop
Advanced Diagnostic Bronchoscopy Workshop
When: March 23-24, 2018
Where: Fort Lauderdale, FL
Program Director: Atul C. Mehta, MD, FACP, FCCP, MD
Program Type: Educational seminar (postgraduate may include physicians in practice and trainees),
Hands-on workshop
Website: http://ccfcme.org/gobronch
3rd Annual Lung Cancer Update: Advances in Screening, Diagnostics and Therapeutics
When: April 13, 2018
Where: William and Ida Friday Center, UNC Chapel Hill, Chapel Hill, NC
Program Director: Lonny Yarmus, DO, FCCP and Jason Akulian, MD, MD
Program Type: Educational seminar (postgraduate may include physicians in practice and trainees),
Hands-on workshop, Conference (didactic lectures)
Ibero-American Symposium on Basic and Advanced Bronchoscopy (SIBBA 2018)
When: April 13-14, 2018
Where: Centro de Convenciones Torre AR, Bogota, Colombia
Program Director: Adnan Majid, MD
Program Type: Educational seminar, Hands-on workshop, Conference (didactic lectures)
Website: http://www.sibbaneumo.com